Pyogenic liver abscess as an extra-intestinal manifestation of pediatric Crohn’s disease
Article information

Abstract
Crohn’s disease (CD) is a type of inflammatory bowel disease (IBD) characterized by chronic granulomatous inflammation of any part of the body, primarily the gastrointestinal (GI) tract, and is increasing in incidence worldwide. As CD is a systemic disease, the features of CD typically manifest in the GI tract; however, a variety of extra-intestinal manifestations, such as the involvement of joints, skin, and eyes may also occur. Although pyogenic liver abscess itself is rare in the general population (approximately 3–5 per 100,000 hospital admissions), it is also an unusual and rare presentation in pediatric CD patients. In this report, we present a case of pyogenic liver abscess in a 7-year-old female CD patient and discuss the clinical features, laboratory findings, imaging studies, and pathologic report of liver biopsy.
INTRODUCTION
Crohn’s disease (CD) is a chronic inflammatory disease that is characterized pathologically by chronic mucosal inflammation and non-caseating granulomas. This process most frequently affects the terminal ileum; however, it may involve any part of the gastrointestinal (GI) tract. The affected area shows a transmural pattern of inflammation, which may be in discontinuity, demonstrating skip lesions.
Although the common features of CD typically manifest in the GI tract, a variety of extra-intestinal manifestations (EIM), such as joint, skin, eye, and hepatobiliary involvement may also occur [1]. EIMs are typically present in 15% to 20% of ulcerative colitis patients and in 20% to 30% of CD patients [2,3], and observed to most frequently affect joints, such as peripheral/axial arthropathies (range, 10% to 35%), followed by the skin, such as erythema nodosum (2% to 20%), pyoderma gangrenosum (0.5% to 2%), Sweet’s syndrome, and aphthous stomatitis [1]. Hepatobiliary EIMs, including primary sclerosing cholangitis (from 0 to 1.3 per 100,000 person/year and 0 to 16.2 per 100,000 people [4]), hepatitis (chronic, active, granulomatous), hepatic abscess, such as pyogenic liver abscess (PLA), hepatic cirrhosis, bile duct carcinoma, fatty liver, and cholelithiasis [5] are some of the rare EIMs in patients with inflammatory bowel disease (IBD) patients. Among EIMs in CD, hepatobiliary involvement, such as cholelithiasis, primary sclerosing cholangitis, and pericholangitis are well documented; however, PLA is rare.
Usually, the incidence of PLA in the general population increases in patients with diabetes mellitus, hepatobiliary diseases, pancreatic diseases, intra-abdominal infections, colorectal cancer, and hepatobiliary and pancreatic system interventions. On the other hand, PLA presents and manifests differently in patients with IBD. A retrospective cohort study in Taiwan demonstrated that the incidence of PLA in patients with IBD was 6.72 per 10,000 person-years, with a 1.46-fold increased risk for PLA compared with the general population [6,7]. According to most PLA case reports, unlike the general population, IBD patients appear to develop PLA at a younger age and are more likely to develop multiple lesions [8].
In this report, we detailed the case of a 7-year-old female patient who presented with PLA during treatment for CD. We also reviewed PLA as an EIM in a pediatric CD patient and discussed its management.
CASE REPORT
A previously healthy 7-year-old female patient visited the pediatric primary outpatient clinic due to an unexplained fever that lasted for approximately 1 month without any GI symptoms. As the fever persisted despite treatment with oral antibiotics, the patient was admitted at another hospital for fever focus evaluation. Although the neck ultrasonography (US) and bone scan results were normal, initial abdomen computer tomography (CT) showed thickening of the ileal wall and an elevated fecal calprotectin value to 2,057 mg/kg, which were highly suggestive of IBD.
Even though the patient showed no GI symptoms, previous clinicians decided to conduct endoscopy to confirm the diagnosis of IBD. Although the results of the esophagoduodenoscopy were normal, colonoscopy results showed multiple small ulcers from the terminal ileum to the rectum with a perianal skin tag (Fig. 1). Additionally, the pathologic results of colon biopsy showed chronic colitis with granuloma formation, meeting the criteria for the diagnosis of CD. As treatment, the patient was started on methotrexate (MTX) treatment (7.5 mg every 1 week [9.37 mg/m2]), and the fever was observed to resolve. However, in spite of 5 months of MTX treatment, the patient showed intermittent prolonged fever with no other GI symptoms for a month, again leading to a visit to our hospital’s outpatient clinic for a secondary opinion of the treatment plan.
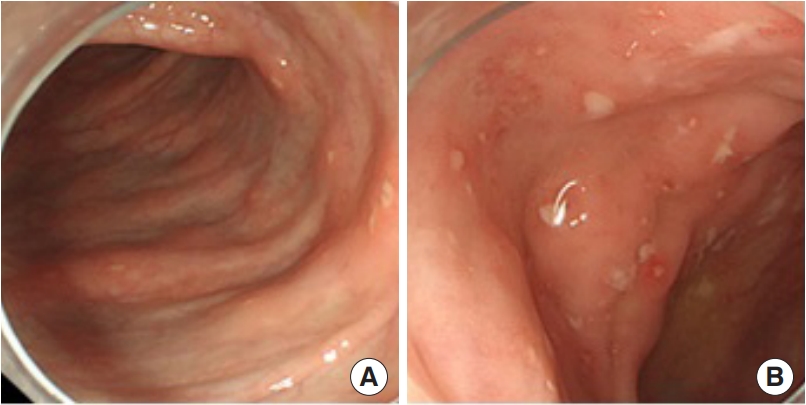
Colonoscopic finding of the case, meeting the criteria for the diagnosis of Crohn’s disease. (A) Small aphthous ulcerations arranged in a longitudinal fashion. (B) Diffuse hyperemic mucosa with several small aphthous ulcerations and a few tiny erosions in ascending colon.
After admission, we performed several tests to evaluate the extent and severity of chronic inflammation of the bowel. The initial Pediatric Crohn’s Disease Activity Index (PCDAI) score was 5, and the physical examination findings were non-specific with no stomatitis nor oral ulcers. For laboratory test, hemoglobin was subnormal level with 11.2 g/dL, hematocrit was 35.0%, on the other hand, C-reactive protein level was 0.23 mg/dL, and the erythrocyte sedimentation rate level rose to 43 mm/hr, with normal α-fetoprotein and serum albumin (4.3 g/dL). Other laboratory blood test results are described in Table 1. The fecal calprotectin value was 100.4 mg/kg, which decreased compared to the initial value; however, it was observed to be still slightly above the upper normal limit (reference range, 0 to 50 mg/kg). Additionally, we performed magnetic resonance enteroclysis to evaluate the activity of disease and found mild wall thickening and mucosal enhancement at the ileocecal valve, terminal ileum, and pelvic ileum. There was no evidence of stricture of bowel wall, perforating complication, perianal fistula, or signs of inflammation.

Complete admission labs of the comprehensive metabolic panel and complete blood count
However, multiple variable sized hepatic masses (more than 10 masses in number, maximum 3 cm in size) were presented, which were previously not observed in the initial CT findings (Fig. 2). These masses were homogenously hyperintense, and predominantly located peripherally. The lymph nodes at the portal hepatis were not remarkable, and the biliary tree showed no enlargement. These multiple hepatic masses required differential diagnosis for hepatic granuloma as an EIM of CD, with pyogenic hepatic abscess and peliosis hepatitis due to drug toxicity. US-guided liver biopsy was performed and the pathologic results (Fig. 3) showed non-caseating granumloma with dense fibrosis with mixed inflammation, histiocytic aggregation, and central necrosis, which may be consistent with PLA. Additional gram stain culture and fungus culture showed no growth of organisms. Additionally, there was no specific microorganisms in the biopsy sample. The patient had no previous history of recurrent infection, including oral candidiasis or acute otitis media, and her complete blood count was unremarkable, indicating low evidence of immunodeficiency. The patient had no other risk factors for liver abscess, the pathological findings and blood laboratory test results showed that there was a low possibility of systemic infection or inflammation sign. Therefore, the PLA was determined to be caused by EIM of CD. Instead of adding antibiotics for the liver abscess, we escalated the CD treatment by increasing the dose of MTX (7.5 mg [9.37 mg/m2] to 10 mg [11.11 mg/m2] every 1 week) and adding infliximab (intravenously infused 5 mg/kg) as an anti-tumor necrosis factor (TNF) α agent and mesalazine (46 mg/kg/day) as 5-aminosalicylic acid.

(A) Magnetic resonance enteroclysis (axial veiw): mild chronic inflammatory bowel change involving the ileocecal valve, terminal, and pelvic ileum. No demonstrable perianal fistula/inflammation and multiple variable-sized heptic mass (arrow), maximum size of 15.26 mm in axial view. (B) Magnetic resonance enteroclysis (coronal view): multiple variable-sized heptic mass, maximum size of 29.30 mm in coronal view.

Patient′s liver biopsy specimen showing a non-caseating granuloma: dense fibrosis with mixed inflammation, histhiocytic aggregation, and central necrosis, which can be consistent with pyogenic liver abscess (H&E, ×100).
An abdominal US was performed 9 months after infliximab was administered, and it was confirmed that all liver abscesses had improved without any other complications (Fig. 4). These improvements demonstrated that liver abscesses, which were EIMs, were also treated during the treatment of CD with infliximab. This study was approved by the Institutional Review Board (IRB) of Samsung Medical Center (IRB No. 2023-08-116). Written informed consent was obtained from the patient.
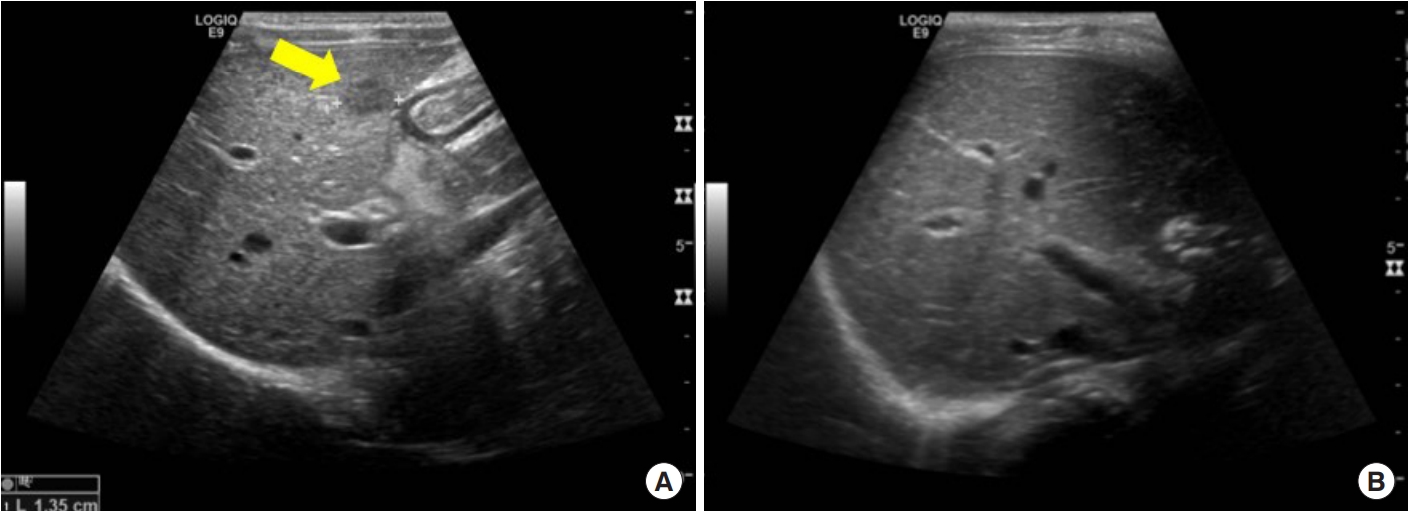
(A) The arrow shows one of the abscesses in the liver at initial ultrasonography (September 2022). (B) Nine months later, all the abscesses were treated with dose escalation of methotrexate and the administration of infliximab and mesalazine (June 2023).
DISCUSSION
The pathogenesis of EIMs in IBD is not yet fully understood; however, some recent studies have suggested that immunologic derangement of the GI mucosa may trigger other immune responses of extra-intestinal organs (i.e., joints, skin, hepatobiliary tract) [5]. In patients with EIM, it is important to know the characteristics of EIM and disease progression early. This is because clinician’s treatment decisions may differ and consequently affect long-term outcomes and complications. The management of EIM should be multidisciplinary and should involve specialists in the affected organ system. Although the treatment strategy for EIM in IBD is often empirical, the mainstay of therapy is treatment of the underlying active IBD. Because recent reports supports the hypothesis that the pathogenesis of intestinal and EIM in IBD share, at least in part, a common TNF-dependent mechanism [9].
The management of IBD-associated hepatic abscesses is still challenging, especially in this case where they occupy multiple segments of the liver. Further decisions of interventional or surgical management with or without medical treatment should be considered with the individual condition of the patient. Although not all liver abscesses are septic, they are usually managed with systemic intravenous antibiotics targeting the prevalent organism [10]. In a typical hepatic abscess, the most frequently isolated organisms include Escherichia coli, Klebsiella pneumoniae, Streptococcus viridans, Staphylococcus aureus, and rarely Clostridia spp. [11]. The mainstays of antibiotic treatment include cephalosporin, aminopenicillin, antipseudomonal penicillin, carbapenem, fluoroquinolone, aminoglycoside, and metronidazole [6]. If size of the abscess is more than 2 cm, antibiotic treatment alone is reported to be insufficient [11] and further surgical (open or laparoscopic drainage) or interventional (percutaneous needle aspiration [PNA] or percutaneous catheter drainage [PCD]) treatment is recommended. PNA is suitable for multiple small lesions to be sample or culture, and PCD is more likely to control large abscesses with less hemodynamic or physiological stress to the patient. Surgical drainage is considered as urgent treatment in case of a ruptured abscess or percutaneous treatment failure. It is reported that surgical treatment results in lower rates of treatment failure in multiloculated abscesses, which are larger than 5 cm in size [12].
In most recent case reports with PLA in CD patients, interventional drainage was carried out concurrently with the systemic antibiotic treatment. However, because our patient had no other plausible evidence of systemic infection except fever, no antibiotic treatment was administered to avoid unnecessary antibiotic exposure.
In conclusion, when a patient with CD presents with multiple liver abscesses, a low inflammatory marker level and no specific organism growth on biopsy culture, we clinicians should carefully consider this as a secondary EIM of CD, which may resolve with treatment of the CD without antibiotic administration.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
AUTHOR CONTRIBUTIONS
Conception or design: YHC, MJK.
Acquisition, analysis, or interpretation of data: JYB, HK, SYK, SYY, TYJ, IH, SA, YZK.
Drafting the work or revising: JYB, MJK, YZK.
Final approval of the manuscript: MJK, YZK.