INTRODUCTION
Osteoporosis is a huge burden of the elderly population that annually causes millions of fractures worldwide [1]. In addition, osteoporosis has close relationship with systemic vascular diseases such as ischemic stroke. Ischemic stroke and osteoporosis have mutual relationship in that osteoporosis could deteriorate by stroke and stroke patients with osteoporosis showed poor clinical outcome [2-4]. A resent epidemiologic study revealed that osteoporosis was associated with the risk of ischemic stroke and accompanied meta-analysis also verified the association between osteoporosis and the risk of ischemic stroke [5].
Osteoporosis also had association with cerebral small vessel disease (SVD), a important cause of ischemic stroke. A recent population-based study showed osteoporosis have an association with cerebral SVD [6]. Other study demonstrated the association between osteoporosis and cerebral white matter changes conducted based on computed tomography (CT) findings [7]. Although the rating scale of cerebral white matter changes applicable to both CT and magnetic resonance imaging (MRI) was available, MRI is still superior in sensitivity especially for detecting small sized changes [8]. Thus, more detailed validations using MRI is requested.
Cerebral white matter hyperintensity is one of the important MRI findings of cerebral SVD [9]. This study aimed to investigate the association between osteoporosis and cerebral SVD, by analyzing correlation of bone mineral density (BMD) and severity of cerebral white matter hyperintensity on MRI.
METHODS
Subjects
Data were extracted from a prospectively collected hospital-based stroke registry (Korea University Stroke Registry-Guro arm; KUSR-G) from January 2008 to September 2014. Details of KUSR were presented in elsewhere [10]. In brief, KUSR have collected the data about acute stroke patients within seven days from the onset of the stroke such as demographic data, vascular risk factors, laboratory findings, and imaging features. Diagnosis of stroke is based on focal neurological symptoms with relevant brain imaging findings. Among the patient registered in KUSR during study period, we selected the patients who met the following criteria; age ≥ 65 years, measurement of BMD, and available fluid attenuated inversion recovery (FLAIR) images on MRI. We sequentially excluded patients who had been prescribed for anti-osteoporotic medications such as alendronate, cholecalciferol, calcitriol, calciumcitrate, or calciumcarbonate. The study protocol was approved and supervised by the Institutional Review Boards of Korea University Medical Center (KUGH-15111). Informed consent was waived by the committee because of the retrospective study design.
Bone densitometry and magnetic resonance images
BMD was measured by dual-energy X-ray absorptiometry (Hologic Discovery A, Belford, MA, USA) for lumbar spine and presented as T-score: T-score= (individual BMD–reference BMD)/reference SD. MRI examination was performed using 1.5 Tesla magnetic resonance (MR) equipment (Sonata, Siemens, Erlangen, Germany) or 3.0 Tesla MR equipment (TrioTim, Siemens). All patients underwent FLAIR imaging (TR 10,000 ms, TE 95 ms, slice thickness 5 mm, FOV 384× 218, no gap for 3.0 Tesla MR; or TR 8,000 ms, TE 108 ms, slice thickness 5 mm, FOV 256 × 192, no gap for 1.5 Tesla MR).
Measurement of white matter hyperintensity on MRI
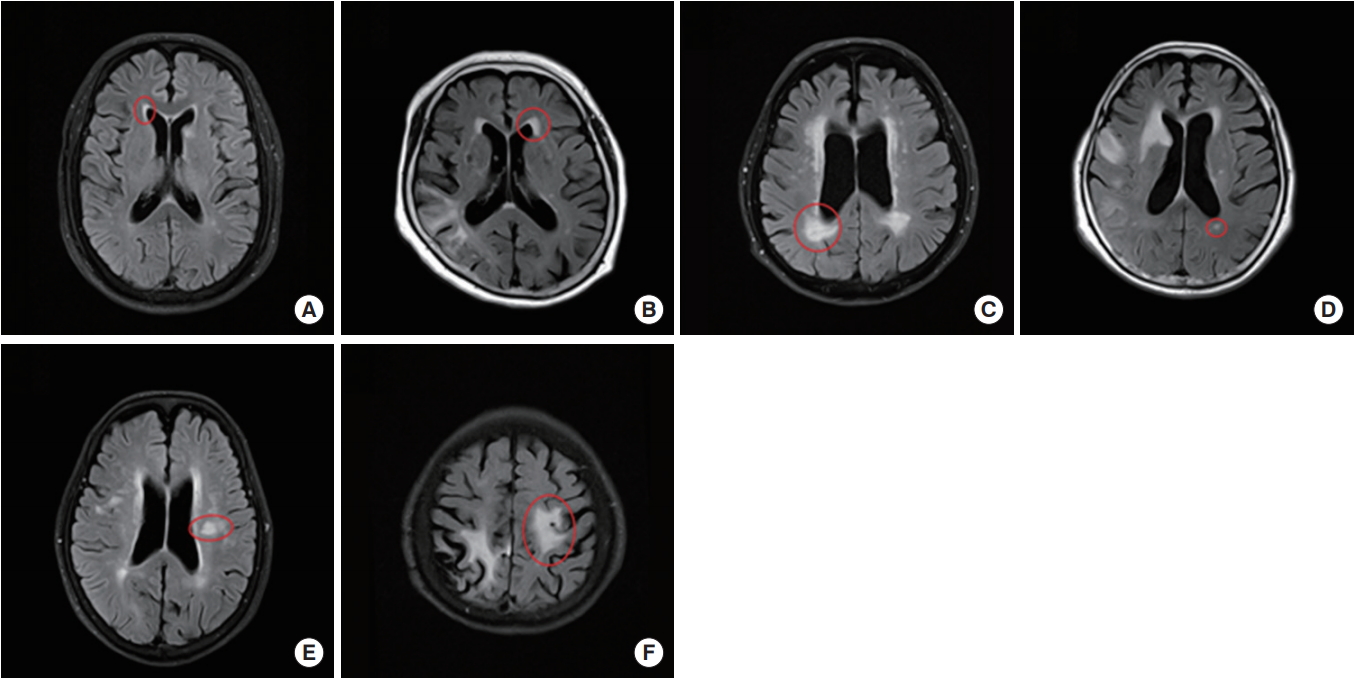
White matter hyperintensity was assessed using previously published semiquantitative scale (Fig. 1) [11,12]. FLAIR image was used for the assessment and the hyperintensity was classified into two categories, those in periventricular white matter and those in deep white matter. When a periventricular cap or band was found, those lesions were defined as periventricular white matter hyperintensity (PWMH). The size of the cap was measured along the longest length from the anterior or posterior horn on a perpendicular axis. The size of the band was measured along the longest length from the lateral wall of the ventricle on the horizontal axis. Both cap and band were rated as P1 ( < 5 mm), P2 (5 to 9 mm), or P3 (≥ 10 mm). Deep white matter hyperintensity (DWMH) was defined as white matter hyperintensity lesion found above the second cut from the upper margin of the ventricle on FLAIR images, or close to the lateral ventricle with normal white matter between them. DWMH was rated as D1 (small and large foci, < 10 mm), D2 (beginning of a confluent lesion, 10 to 24 mm), or D3 (confluent lesion, ≥ 25 mm). Infarction lesions, both acute and chronic state, were excluded from the assessment. Lacunar infarction was also excluded, defined as following; size 3 to 15 mm, T2 high signal, FLAIR low signal with gliotic rim, and T1 low signal [9].
Statistical analysis
The differences of clinical characteristics between subgroups were tested with one way analysis of variance (ANOVA) for continuous variables and chi-square test for categorical variables. To investigate associations between the clinical factors and cerebral white matter hyperintensity, both univariable and multivariable ordinal regression analysis were performed. In multivariable ordinal regression analysis model, variables with P < 0.10 in univariable analysis and clinically important factors such as BMD, alkaline phosphatase (ALP), phosphorus, calcium, and glomerular filtration rate (GFR) were included and backward elimination method was used. All statistical analyses were performed using SPSS version 20.0 (IBM Co., Armonk, NY, USA), R language version 3.01 (R Foundation for Statistical Computing, Vienna, Austria), or SAS version 9.1 (SAS Institute Inc., Cary, NC, USA), and P-values < 0.05 were regarded as significant.
RESULTS
Finally, 408 patients were included in the study; 75.37± 6.17 years old and 213 (52.2%) were male. Mean BMD T-score was –2.439± 1.15 and 202 (49.5%) had osteoporosis, T-score lower than –2.5. Distribution of PWMH subgroup was as follows; 124 for grade 1, 155 for grade 2, and 129 for grade 3. Distribution of DWMH subgroup was as follows; 203 for grade 1, 138 for grade 2, and 67 for grade 3. In comparison of clinical characteristics among PWMH subgroups, age, height, BMD, hypertension history, atrial fibrillation (AF) history, triglyceride, homocysteine, ALP, and GFR were significantly different. In comparison of clinical characteristics among DWMH subgroups, age, sex, height, and BMD were significantly different (Table 1).
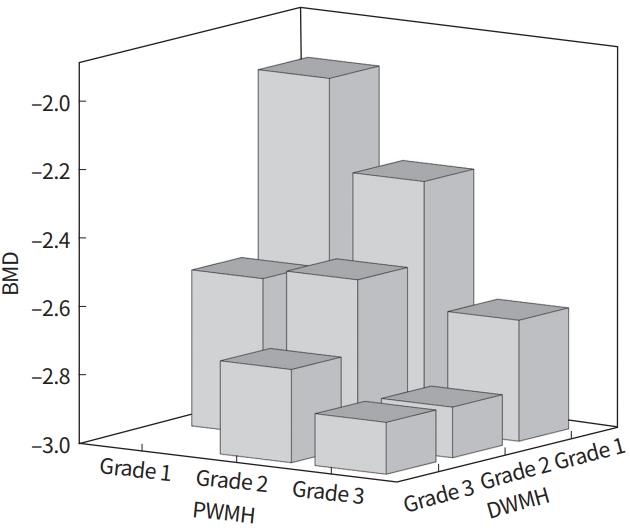
In univariable regression analysis of PWMH as a response variable, age, sex, weight, height, BMD, hypertension history, AF history, GFR, and homocysteine showed significant association with P-value less than 0.1 (Supplementary Table 1). In univariable regression analysis of DWMH as a response variable, age, sex, weight, height, BMD, hypertension history, AF history, total calcium, and GFR showed P-value less than 0.1 (Table 1). In multivariable regression analysis, BMD was significantly correlated with both PVMH (odd ratio [OR], –0.416; 95% confidence interval [CI], –0.654 to –0.178; P= 0.001) and DVMH (OR, 0.306; 95% CI, –0.546 to –0.067; P= 0.012) (Table 2). Changes of PWMH and DWMH grades exert synergistic effect on BMD (Fig. 2). In addition, several factors showed significant correlations; old age and high serum homocysteine for high PWMH grade; old age, AF history, and high serum total calcium for high DWMH grade.
DISCUSSION
In the present study, severity of cerebral white matter hyperintensity on MRI showed significant associations with BMD, compatible results with the previous study. Previous study showed significant association between presence of osteoporosis and cerebral SVD on CT [7]. Although other previous study stated no significant correlation between SVD and low BMD, the study used phalynx rather than femur neck as measuring site of BMD [13]. Because phalynx is not a recommended site for BMD measuring to assess osteoporosis in clinical practice, BMD measured in phalynx maybe insufficiently reflect the presence of osteoporosis [14].
It is suggested that sharing of risk factor might explain the association between osteoporosis and cerebral SVD [7]. Traditionally, cerebral SVD that refers to atherosclerosis has been known as having risk factors such as aging, hypertension, diabetes mellitus, dyslipidemia, smoking, or homocysteine [15]. Osteoporosis has several risk factors similar to cerebral SVD in part, like smoking and old age. However, in this study, the association between cerebral white matter hyperintensity and BMD was independent of such risk factors, thus the association could not be explained by risk factors sharing. Although the underlying pathophysiologic mechanisms between osteoporosis and cerebral SVD are still on debate, one of the possible explanations is that osteoporosis-related abnormal calcium metabolism could increase vascular calcification and arterial wall stiffness [5,16]. Vascular calcification has been suggested as a marker of cerebral SVD in recent observations [17,18]. The association may also be explained by common pathophysiology of the two conditions. Atherosclerosis, a main pathology of cerebral SVD, and osteoporosis are known to have common pathogenesis like bone morphogenetic proteins, the receptor activator of nuclear factor-kappaB ligand (RANKL)/RANK/osteoprotegerin (OPG) pathway, matrix Gla protein (MGP) and vitamin K [19]. Low vitamin D level also is known to be associated with increased vascular risk [20].
If osteoporosis is an independent risk factor of cerebral SVD, we can assume that treatment of osteoporosis reduces the occurrence or progression of cerebral SVD. However, such concept should be considered with caution. Two well-established agents for treating osteoporosis, bisphosphonate, and calcium, showed a dissimilar influence to atherosclerosis. There has been no consensus about the effect of bisphosphonate on atherosclerosis. Several observational studies demonstrated that bisphosphonate treatment had benefit on reducing the risk of cardiovascular disease such as myocardial infarction or stroke [21,22]. Bisphosphonate has been suggested to reduce cardiovascular disease by the following mechanisms; inhibition of intimal hyperplasia, macrophage-related inflammation, and vascular calcification [22,23]. However, recent meta-analysis showed different results that bisphosphonate do not act as beneficial or harmful factor on atherosclerosis [24]. Meanwhile, calcium supplements may be harmful to cardiovascular disease [25,26]. Contrast to daily calcium intake dose, artificial calcium supplements lead to significant increase of serum calcium level. The increased calcium level is associated with increased cardiovascular risk [25,27,28]. Whether active treatment of osteoporosis reduces the risk of cerebral SVD is not clear and careful approach is needed.
In addition to BMD, several factors were associated with cerebral SVD. Age was independent risk factor for both PWMH and DWMH, as reported in previous study [29]. AF was inversely correlated with DWMH (P= 0.011; OR, –0.634). Although statistically not significant, PWMH also showed tendency of negative association with AF (P= 0.071; OR, –0.436). The results can be explained by the following. The study was performed with acute symptomatic stroke patients. AF is a major cause of cardioembolic stroke, and patients with cardioembolic stroke have smaller cerebral white matter hyperintensity volume than those with large artery atherosclerosis or small vessel occlusion [30,31]. Homocysteine showed significant association with PVMH but not with DVMH. In the contrast, serum calcium level is associated with DVMH only. Discrepancy of significant association factors between PWMH and DWMH may indicate that the two categories have different pathomechanism in part, which is not clearly identified, and reserved for future investigation.
The present study has several limitations. First, the study population consisted of a single-race, was selected from hospitalized symptomatic stroke patients and healthy subjects were not included. Thus there are some limitations to generalize the results. Second, subjects taking osteoporosis medications were excluded for the study. The strict inclusion criteria was unavoidable due to more homogeneous study populations; however, subjects with severe or symptomatic osteoporosis may be eliminated from the study and it can attenuate the results. Finally, MRI equipment used for the study was not identical to each other, one was 1.5 Tesla and the other was 3.0 Tesla. Because measurement of cerebral white matter intensities is a precision task and requires high resolution images, heterogeneity of MRI equipment may influence to measured size of cerebral white matter intensities. However, possible missing or mis-sized lesions on low tesla MRI are often small-sized; hence, they do not significantly influence to grading of cerebral white matter hyperintensity, because the grade in the study was decided by size of biggest lesion [32].
In conclusion, low BMD was associated with a high severity of cerebral white matter hyperintensity in elderly Asian stroke patients. This association was independent of a shared etiology of osteoporosis and cerebral SVD. Osteoporosis could be linked to dementia or stroke through cerebral SVD, it would be important to screen osteoporosis in advance. But the effect of osteoporosis treatment on cerebral SVD is still on debate and further longitudinal studies are requested.