INTRODUCTION
Diabetes mellitus is an established risk factor for both incident and recurrent stroke [1,2]. However, intensive glycemic control does not prevent risk of stroke in diabetic patients [3]. Many large randomized controlled trials of antidiabetic drugs have been published recently, but since occurrence of stroke was not a prespecified primary endpoint, the effect of individual antidiabetic drug on the risk of stroke might be overlooked. In this article, we review the evidence currently available for the relation between blood glucose levels and risk of stroke, and clarify the effect of individual antidiabetic drugs on stroke prevention. We then propose potential therapeutic strategies to combine antidiabetic drugs to maximize cardiovascular benefits, and mitigate side effects in ischemic stroke patients with type 2 diabetes.
BLOOD GLUCOSE AND RISK OF STROKE
Diabetes mellitus and risk of stroke
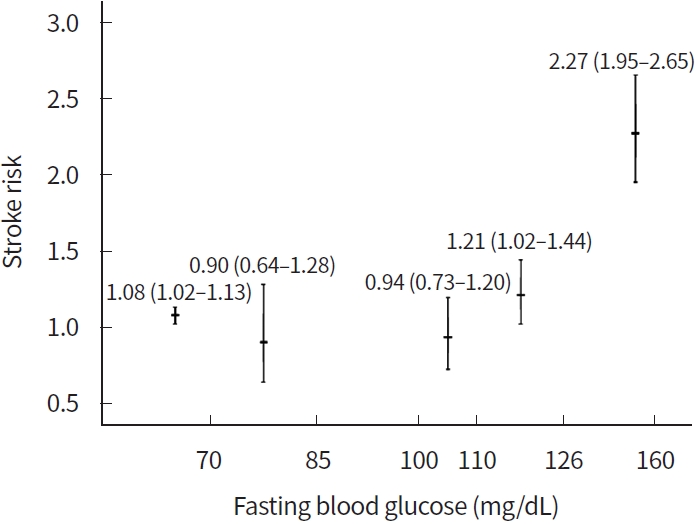
A meta-analyses including data for over 530,000 people from 102 prospective studies suggested that comparing people with diabetes versus those without, future risks were higher for ischemic stroke (hazard ratio [HR], 2.27; 95% confidence interval [CI], 1.95 to 2.65), hemorrhagic stroke (HR, 1.56; 95% CI, 1.19 to 2.05), and unclassified stroke (HR, 1.84; 95% CI, 1.59 to 2.13) after adjustment for age, sex, smoking status, body mass index, and systolic blood pressure [4]. For people with diabetes mellitus, future risks for ischemic stroke were especially higher in women, in people with a higher body mass index, and in people aged between 40 and 59 years [4].
Prediabetes and risk of stroke
The growing obesity epidemic in the United States of America has been linked with a surge in rates of prediabetes [5]. People with prediabetes harbor the same vascular risk factors (hypertension, dyslipidemia, obesity, physical inactivity, insulin resistance, and inflammation) that place people with diabetes mellitus at a high risk of major cardiovascular events [6]. In eight studies with information about fasting glucose 100 to 125 mg/dL, the pooled estimate did not show increased risk of stroke after adjustment for established cardiovascular risk factors (relative risk [RR], 1.08; 95% CI, 0.94 to 1.23) [7]. In five studies with information about fasting glucose 110 to 125 mg/dL, the pooled estimate showed an increased risk of stroke after adjustment for established cardiovascular risk factors (RR, 1.21; 95% CI, 1.02 to 1.44) [7]. In eight studies with information about impaired glucose tolerance or combination of impaired fasting glucose and impaired glucose tolerance, the pooled estimate showed an increased risk of stroke after adjustment for established cardiovascular risk factors (RR, 1.26; 95% CI, 1.10 to 1.43) [7]. In three studies that provided information on participants with fasting glucose of 100 to 109 mg/dL, the pooled estimate did not show an increased risk of stroke (RR, 0.94; 95% CI, 0.73 to 1.20) [7].
Low fasting glucose and risk of stroke
Since glucose is a necessary body nutrient, and blood glucose concentration is regulated by various hormones within a narrow range in the body [8], it is conceivable that fasting blood glucose lower than a certain threshold may be associated with harmful effects among people without baseline diabetes mellitus and cardiovascular disease. A meta-analysis found that in studies using fasting glucose < 85 mg/dL as cutoff, the pooled estimate did not show an increased risk of total stroke (HR, 0.90; 95% CI, 0.64 to 1.28), ischemic stroke (HR, 1.03; 95% CI, 0.94 to 1.12), or hemorrhagic stroke (HR, 0.98; 95% CI, 0.88 to 1.09) [9]. However, approximately 5% of people without diabetes and cardiovascular disease at baseline have fasting blood glucose levels < 70 mg/dL and these individuals harbor greater hazards of future total stroke (HR, 1.08; 95% CI, 1.02 to 1.13) and ischemic stroke (HR, 1.06; 95% CI, 1.01 to 1.10), as compared to individuals with a normal blood glucose level [9].
The relationship between fasting blood glucose levels and stroke risk is presented in the Fig. 1.
ANTIDIABETIC DRUGS FOR STROKE PREVENTION
Metformin for stroke prevention
In the UK Prospective Diabetes Study (UKPDS), a secondary analysis compared the 342 patients allocated metformin with 951 patients allocated intensive blood-glucose control with chlorpropamide, glibenclamide, or insulin and found metformin showed a greater effect than chlorpropamide, glibenclamide, or insulin for reducing stroke risk (RR, 0.59 vs. 1.14, P= 0.03) among diabetic patients who were overweight [10]. However, a 10-year follow-up of UKPDS did not show a significant risk reduction for stroke in people assigned to metformin group [11]. Also, all of the metformin-treated subjects were overweight or obese, and the number receiving this treatment (n= 342) would be considered relatively small for a cardiovascular outcomes study by today’s standards. Finally, a Cochrane review suggested no clear evidence about whether metformin monotherapy compared with behavior change, no intervention, or other glucose-lowering drugs influences patient-important outcomes, including nonfatal stroke [12].
Sulfonylureas for stroke prevention
In the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial, gliclazide use compared with placebo had no effect on non-fatal stroke [13]. A Cochrane review suggested inconclusive evidence about whether metformin plus sulfonylurea compared with metformin plus another glucose-lowering intervention showed benefit or harm for most patientimportant outcomes, including nonfatal stroke [14]. On the other hand, in a Bayesian meta-analysis of both randomized controlled trials and cohort studies, the risk of stroke was significantly higher in sulfonylurea users than users taking other anti-diabetic agents [15].
Glinides for stroke prevention
The Nateglinide and Valsartan in Impaired Glucose Tolerance Outcomes Research (NAVIGATOR) trial showed that among people with prediabetes, one or more cardiovascular risk factors, or known cardiovascular disease, nateglinide compared with placebo neither decreased or increased the risk of nonfatal or fatal stroke (HR, 0.89; 95% CI, 0.69 to 1.15) [16].
Pioglitazone for stroke prevention
In a subgroup analysis of diabetic patients with prior stroke in the PROspective pioglitAzone Clinical Trial In macroVascular Events (PROactive), pioglitazone compared with placebo was associated with a lower risk of fatal or nonfatal stroke (HR, 0.53; 95% CI, 0.34 to 0.85) [17]. In the Insulin Resistance Intervention after Stroke (IRIS) trial involving patients without diabetes but with insulin resistance along with a recent history of ischemic stroke or transient ischemic attack, pioglitazone compared with placebo reduced the risk of stroke or myocardial infarction (HR, 0.76; 95% CI, 0.62 to 0.93) [18]. A meta-analysis including three randomized controlled trials with 4,980 participants suggested that pioglitazone use in stroke patients with insulin resistance, prediabetes, and diabetes mellitus was associated with lower risks of recurrent stroke (HR, 0.68; 95% CI, 0.50 to 0.92) and future major cardiovascular events (HR, 0.75; 95% CI, 0.64 to 0.87) [19].
Dipeptidyl peptidase-4 inhibitors for stroke prevention
The Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS) study showed that among patients with type 2 diabetes and established cardiovascular disease, adding sitagliptin to usual care did not decrease or increase the risk of stroke (HR, 0.97; 95% CI, 0.79 to 1.19) [20]. The Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus (SAVOR)–Thrombolysis in Myocardial Infarction (TIMI) 53 trial showed that among patients with type 2 diabetes who had a history, or at risk for, cardiovascular disease, adding saxagliptin did not decrease or increase the risk of ischemic stroke (HR, 1.11; 95% CI, 0.88 to 1.39) [21]. The Cardiovascular and Renal Microvascular Outcome Study With Linagliptin (CARMELINA) trial showed that among adults with type 2 diabetes and high cardiovascular and renal risk, linagliptin compared with placebo did not decrease or increase the risk of nonfatal or fatal stroke (HR, 0.91; 95% CI, 0.67 to 1.23) [22]. A meta-analysis of 36 randomized trials suggested there was no significant difference in stroke risk (RR, 1.02; 95% CI, 0.88 to 1.17) with the use of dipeptidyl peptidase-4 inhibitors, compared with placebo [23].
Sodium-glucose co-transporter 2 inhibitors for stroke prevention
The Empagliflozin Cardiovascular Outcome Event Trial in Type 2 diabetes Mellitus Patients (EMPA-REG OUTCOME) trial showed that among type 2 diabetic patients at high risk for cardiovascular events, empagliflozin compared with placebo did not significantly decrease or increase the risk of nonfatal or fatal stroke (HR, 1.18; 95% CI, 0.89 to 1.56) [24]. The numeric difference in stroke between empagliflozin and placebo in the modified intent-to-treat analysis was primarily due to 18 patients in the empagliflozin group (vs. 3 on placebo) with a first event > 90 days after last taking of study drug. In a sensitivity analysis based on events during treatment or ≤90 days after last dose of drug, the HR for stroke with empagliflozin versus placebo was 1.08 (95% CI, 0.81 to 1.45) [25]. The Canagliflozin Cardiovascular Assessment Study (CANVAS) Program showed that among patients with type 2 diabetes and an elevated risk of cardiovascular disease, canagliflozin compared with placebo did not decrease or increase the risk of fatal or nonfatal stroke (HR, 0.87; 95% CI, 0.69 to 1.09) [26]. The Dapagliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction 58 (DECLARE–TIMI 58) trial showed that among patients with type 2 diabetes who had or were at risk for atherosclerotic cardiovascular disease, dapagliflozin did not decrease or increase the risk of stroke (HR, 1.01; 95% CI, 0.84 to 1.21) [27]. A meta-analysis of these 3 large randomized controlled trials suggested sodium-glucose co-transporter 2 (SGLT-2) inhibitors compared with placebo had no effect on stroke (HR, 0.97; 95% CI, 0.86 to 1.10) [28].
Glucagon-like peptide-1 receptor agonists for stroke prevention
The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial showed that among patients with type 2 diabetes and high cardiovascular risk, use of liraglutide compared with placebo did not significantly reduce the risk of stroke (HR, 0.86; 95% CI, 0.71 to 1.06) [29]. The preapproval Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type 2 Diabetes (SUSTAIN-6) showed that among type 2 diabetic patients at high risk for cardiovascular events, subcutaneous semaglutide once weekly, compared with placebo, reduced the rate of nonfatal stroke (HR, 0.61; 95% CI, 0.38 to 0.99) [30]. The Researching Cardiovascular Events with a Weekly Incretin in Diabetes (REWIND) trial showed that among type 2 diabetes with either previous cardiovascular disease or cardiovascular risk factors, subcutaneous dulaglutide once weekly, compared with placebo, reduced the rate of ischemic stroke (HR, 0.75; 95% CI, 0.59 to 0.94) and similar effects for dulaglutide on stroke were observed in people with or without a history of stroke or transient ischemic attack [31]. The Exenatide Study of Cardiovascular Event Lowering (EXSCEL) trial showed that among type 2 diabetic patients with or without previous cardiovascular disease, subcutaneous injections of once-weekly exenatide compared with placebo did not significantly reduce the risk of nonfatal stroke (HR, 0.85; 95% CI, 0.70 to 1.03) [32]. The Peptide Innovation for Early Diabetes Treatment (PIONEER) 6 trial showed that among diabetic patients at high cardiovascular risk, once-daily oral semaglutide compared with placebo did not significantly reduce the risk of nonfatal stroke (HR, 0.74; 95% CI, 0.35 to 1.57) [33]. A network meta-analysis evaluating all antidiabetic drugs suggested the risks of stroke were lower with use of subcutaneous semaglutide and dulaglutide in patients at increased cardiovascular risk who received metformin-based background treatment [34].
Acarbose for stroke prevention
The Acarbose Cardiovascular Evaluation (ACE) trial showed that among Chinese patients with coronary heart disease and impaired glucose tolerance, use of acarbose compared with placebo did not reduce the risk of fatal or nonfatal stroke (HR, 0.97; 95% CI, 0.70 to 1.33) [35]. In a Taiwan nationwide cohort study, acarbose was associated with a borderline higher risk of ischemic stroke (HR, 1.05; 95% CI, 1.00 to 1.10) than metformin and therefore did not support the notion that acarbose should be a first-line antidiabetic agent [36].
Insulin for stroke prevention
In the Outcome Reduction with an Initial Glargine Intervention (ORIGIN) trial, which involved people 50 years of age or older with impaired fasting glucose, impaired glucose tolerance, or early type 2 diabetes in addition to other cardiovascular risk factors, insulin glargine compared with standard care did not decrease or increase the risk of total stroke (HR, 1.03; 95% CI, 0.89 to 1.21) [37].
Antidiabetic drugs that may reduce future stroke risk are presented in the Table 1.
COMBINATION OF ANTIDIABETIC DRUGS FOR SECONDARY STROKE PREVENTION
Since pioglitazone use might be associated with reduced recurrent stroke risk in ischemic stroke patients with insulin resistance, prediabetes, and diabetes mellitus [19], the Taiwan Society of Cardiology and the Diabetes Association of Republic of China (Taiwan) recommend metformin plus pioglitazone for dual therapy in diabetic patients with a history of ischemic stroke [38]. However, a meta-analysis of randomized controlled trials shows that the risks of heart failure, edema and weight gain are higher in patents taking pioglitazone [39]. As shown in a randomized controlled trial, the potential risk of heart failure can be mitigated, even eliminated, by excluding patients with a history of heart failure and using safety algorithms that trigger dose reduction of pioglitazone for excessive weight gain or edema [18]. Still, mild weight gain or edema seems inevitable once pioglitazone is used [18]. It would be helpful if adding another antidiabetic drug to metformin and pioglitazone could mitigate the side effects of pioglitazone and/or potentially maximize cardiovascular protection, without an increase in the risk of hypoglycemia.
Metformin+ pioglitazone+ SGLT-2 inhibitor
A meta-analysis of four randomized controlled trials suggested that compared to pioglitazone alone, an SGLT-2 inhibitor plus pioglitazone improved glycemic control, reduced body weight and lowered blood pressure, without an increased risk of hypoglycemia [40]. Furthermore, SGLT-2 inhibitor use can reduce incident risks of heart failure, cardiovascular death, end stage renal disease, albuminuria, and atrial fibrillation [24,26,27,41-44]. Although SGLT-2 inhibitor use is not associated with reduced risk of stroke, its potential to mitigate the side effects of pioglitazone and its cardio-renal protective effect make it an optimal antidiabetic drug to be added to metformin and pioglitazone in ischemic stroke patients with type 2 diabetes.
Metformin+ pioglitazone+subcutaneous dulaglutide or semaglutide
The Assessment of Weekly AdministRation of LY2189265 (dulaglutide) in Diabetes-1 (AWARD-1) trial showed that among patients treated with metformin and pioglitazone, once-weekly subcutaneously injection of dulaglutide compared with placebo resulted in significantly larger improvements in glycosylated hemoglobin (HbA1c), and percentages of patients achieving target HbA1c goals, as well as significant weight reduction, and no dulaglutide-treated patients reported severe hypoglycemia [45]. Since use of subcutaneous dulaglutide or semaglutide is associated with reduced risk of stroke and major cardiovascular events [30,31,46], and adding subcutaneous dulaglutide or semaglutide to metformin and pioglitazone mitigates the side effects of pioglitazone, improves blood glucose control, but is less likely to increase risk of hypoglycemia, such a combination could be a reasonable therapeutic regimen to be used in ischemic stroke patients with type 2 diabetes.
Suggested strategy for combination of antidiabetic drugs in ischemic stroke patients with type 2 diabetes is presented in Table 2.
CONCLUSION
The risk of stroke is increased among people with diabetes, people without diabetes but with impaired glucose tolerance, people with fasting glucose between 110 and 125 mg/dL, and those with fasting glucose < 70 mg/dL. Among stroke patients with insulin resistance, prediabetes, or diabetes mellitus, pioglitazone use might be associated with a reduced risk of recurrent stroke and major cardiovascular events. Among diabetic patients with increased cardiovascular risk, once-weekly subcutaneous injection of semaglutide or dulaglutide reduces future stroke risk. The combination of metformin, pioglitazone and SGLT-2 inhibitor or combination of metformin, pioglitazone and subcutaneous semaglutide/dulaglutide could be considered as reasonable therapeutic strategies for optimally effective and safe secondary stroke prevention in ischemic patients with type 2 diabetes, pending robust evidence from randomized controlled trials.