INTRODUCTION
Advanced head and neck cancer (HNC) still causes significant cancer mortality from metastasis, even with recent advancements in cancer therapeutics [1,2]. To achieve better outcomes in advanced HNC, multi-modal treatments were developed. These treatments have been proven to be more effective and have become the standard of care [3,4]. Surgery is usually directed for resectable cases in advanced HNC, with the aim of achieving complete resection (R0) orinevitable micro-residual disease (R1), no gross residual disease (R2)[5].
Palliative surgery in cancer treatment involves various forms of interventions in incurable HNC [6-8]. To secure the airway, prophylactic tracheostomy is one of the most common procedures in patients with HNC, and endoscopic or fluorographic gastrostomy is another palliative method to improve patient’ nutrition and quality of life [8]. Palliative tumor surgery (PTS) specifically indicates the removal of cancer tissue to improve patient’ quality of life, but not complete eradication ofthe cancer[9,10].
Apart from palliative surgery, numerous articles have suggested the clinical usefulness of palliative radiation to control cancer-related pain in patients with HNC [11,12]. However, additional palliative radiation cannot always be performed for patients with HNC who have already received heavy irradiation, or for some tumors not responsive to radiation. Radiation can aggravate wound problems (infection, fistula, or bleeding from major vessels) in HNC patients with open cancer wounds.
In addition to improving patient comfort, a tailored palliative surgery can prolong patient survival in some cases [13]. Thus, it is important to refine the surgical indications of PTS for patients with HNC, under the multi-modal treatment strategies. Although radiation treatment has shown the promising palliative effects, few reports have addressed the role of PTS in patients with incurable HNC [11,12]. Thus, this retrospective case review was designed to present the outcomes of PTS in HNC, and to suggest surgical indications for which patients with HNC would most benefit.
METHODS
Study patients
We retrospectively reviewed the electronic medical records of patients who underwent PTS for HNC between 2002 and 2017. We defined PTS as (1) surgical debulking ofthe tumor in the primary site or neck, where complete tumor resection (R0) was not possible or(2) surgery to remove loco-regional tumors in a patient with distant metastasis (M1). Surgical procedures such as tracheostomy for airway maintenance or gastrostomy for nutritional support were excluded from the analysis.
During the 16-year study period, we identified 18 patients among 3,000 HNC surgeries, who met the inclusion criteria. The following clinical information was retrospectively obtained for each patient: age, gender, performance status, primary site,tumor pathology, initial and recurrent tumor-node-metastasis (TNM) stage (according to the American Joint Committee on Cancer [AJCC] 7th edition), treatments, and survival. Performance status was measured using the Eastern Cooperative Oncology Group (ECOG) scale [14]. The protocol of this retrospective study was approved by Institutional Review Board of Samsung Medical Center(IRB No. 2015-06-132), and the requirement for written informed consent was waived.
Outcomes of palliative tumor surgery
For functional outcomes, we focused on pre-surgery to post-surgery changes in pain, diet, respiration, and wound care. Post-operative data were collected at 1 to 2 months after PTS, when the surgical wounds had almost healed. Pain severity was measured using a numeric rating scale (NRS; 0, no pain; 10, maximum) [15]. Open wounds were re-evaluated by medical records and classified as persistent tumor bleeding, pus discharge orfoul odor with associated wound infection.
Swallowing function was categorized based on dietary status in the following groups: tube feeding, oral soft fluid diet, soft blended diet, and normal regular diet (NRD). Regarding airway maintenance, the status of airway in patients was divided into normal patent airway (without tracheostomy) or tracheostomy (including total laryngectomy). Overall survival after PTS was calculated from the time of PTS until the last follow-up or death from any cause.
Statistical analyses
Statistical analysis was performed using SPSS software version 20 (IBM SPSS, Armonk, NY, USA). Patient survival was calculated using the Kaplan-Meier method. Changes in pain scores were compared with a non-parametric paired test (before and after PTS) (McNemar test). The significance level for all statistical comparisons was set at P<0.05.
RESULTS
Patient characteristics and initial treatments
The patient characteristics are summarized in Table 1. Fifteen of the 18 (83%) subjects were male, and the median age was 59 years (range, 35 to 71). Regarding the primary site, the oral cavity ranked first (27.8%) followed by the larynx (22.2%) and unknown primary HNCs (16.7%). Squamous cell carcinoma was the most common histology (72.2%). Six patients (33.3%) had distant metastasis (M1) (five lung and one bone metastasis) and 16 patients (88.8%) had AJCC stage IV cancer at diagnosis. The 66.7% of patients (n=12) experienced recurrence after initial curative treatments (six surgery alone, five surgery with adjuvant radiation or chemoradiation, one definitive radiation). The remaining six patients (33.3%) were managed with initial palliative treatments (three surgery with chemotherapy, two chemoradiation, one surgery with radiation). All patients had stage IV cancer and 12 patients (66.7%) had distant metastasis at the time of PTS.
Clinical consequences of palliative tumor surgery
At the time of PTS, ten patients had metastasis in lung, one in bone, and the other one in the lung and skull base. PTS was performed for the following purposed: (1) debulking of large tumors (55.6%); (2) wound management(22.2%); (3) pain control (11.1%); and (4) improvement of oral swallowing (11.1%) (Table 1).
Three patients were excluded from the survival calculation due to short follow-up duration. Among the 15 patients, eight patients died due to cancer-related problems (53.3%). There were four deaths of cancer-unrelated reasons (heart, respiratory, hepatic failures, and accident), and three were lost to follow-up or censored at the time of data collection. The median overall survival time was 17 months (95% confidence interval, 7.3 to 26.7)in 15 patients who received PTS (Fig. 1).
Although PTS was primarily performed to manage cancer-related pain in only two patients, 17 patients (94.4%) experienced a decrease in pain score after PTS. The mean preoperative NRS score was 3.21 (range, 0 to 8), but it was reduced to 1.14 (range, 0 to 4) after the operation, representing a significant decrease (P=0.013)(Fig. 2).
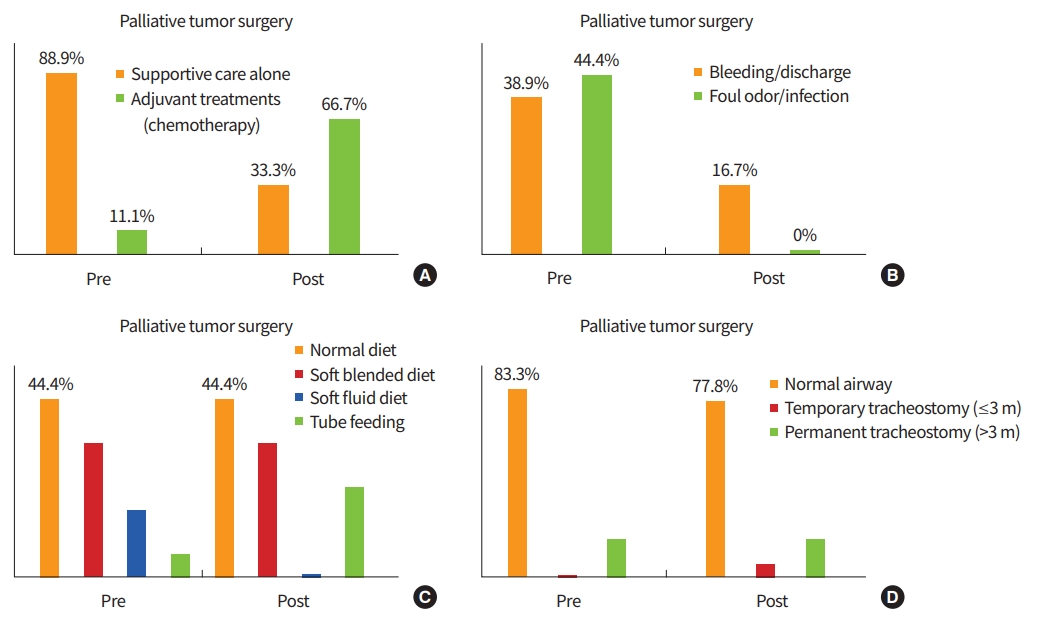
Changes of the clinical variables after PTS are summarized in Fig. 3. Before surgery, 16 patients (88.8%) had received supportive care alone (duration, 1.0 to 7.5 months) without any cancer treatments. However, 10 patients were able to receive chemotherapy or other additional treatments after PTS.
Approximately 40% of the patients suffered from bleeding, discharge, and foul odor due to loco-regional tumor progression. The wound problems were well managed with PTS, suggesting that PTS improved quality of life of these patients.
In addition, we investigated the post-operative changes in diet(swallowing) and respiration. Eight patients (44.4%) were able to take NRD before and after surgery. Fifteen patients (83.3%) had a normal oro-laryngo-tracheal airway before surgery and one additional transient tracheostomy was required with PTS. Overall swallowing and respiratory functions were similar between pre-operative and post-operative status. Rather, those functions were transiently decreased at the immediate post-operative period and then slowly returned to the pre-operative status.
DISCUSSION
Advanced stage HNC at presentation or metastatic/recurrent HNC still signifies a poor patient prognosis, even with recent advances in diagnostic modalities and multi-modal treatments [16]. A longitudinal follow-up study of untreated patients with HNC (91% of whom were in stage IV) showed a median survival of approximately 100 days [17]. Previously, we also reported survival outcomes of HNC patients with distant metastasis, and we found that the median survival of HNC patients with multiple distant metastases of high glucose uptake on positron emission tomography (standard uptake value >6.3) was only 10 months [18]. The symptoms of these patients worsened gradually over a period of a few months, and the patients suffered from physical and psychological distress [9]; thus, many patients needed palliative treatment. Several studies have suggested the clinical usefulness of palliative radiation or chemotherapy in patients with HNC [19-21]; however, few reports have studied the role of PTS in patients with incurable/unresectable HNC [22]. Therefore, we aimed to present the outcomes of palliative surgery for incurable HNC, and to suggest possible surgical indications for PTS.
Palliative treatments in patients with HNC, including gastrostomy and tracheostomy, are designed primarily to relieve pain, support nutrition and secure the airway. Apart from gastrostomy and tracheostomy, PTS in HNC seems to play a minor role in patient management compared with supportive care, chemotherapy, or radiation [23]. Palliative chemotherapy response rate typically range from 20% to 50%; longer survival rates can be achieved depending on the drug regimen [19,21]. There have been conflicting reports about the effects of palliative chemotherapy for HNC on quality of life [20,24]. However, no well-designed randomized clinicaltrial has been undertaken to definitively show a survival benefit of palliative chemotherapy over the best supportive care for these patients [25]. In reality, it appears to be difficult to manage local cancer-related wound problems during chemotherapy.
The primary goal of radiotherapy for patients with incurable HNC is effective palliation, i.e., improved quality of life, symptom relief, and fewer complications, all with minimal toxicity [26]. Numerous studies have suggested that palliative radiotherapy could achieve high rates of symptom relief in HNC patients, even with only marginal or no survival benefit [27-29]. However, loco-regionally advanced HNC represents a significant treatment challenge due to the close proximity of tumors to critical normal tissues, such as the skull base, spinal cord, salivary glands, cranial nerves, major blood vessels and the organs of speech, swallowing,respiration, and hearing [28]. Likewise, significant overlap can exist between the presenting symptoms and radiation-related toxicity, making decisions about palliative radiotherapy challenging. Moreover, high quality evidence is lacking for determining the optimal palliative radiation regimen (time,dose, and fractionation).
It is worth noting that patients with recurrent/metastatic HNC can receive maximal acceptable doses of radiation for surrounding tissue and organs over multiple courses of radiotherapy. Re-irradiation could carry significant potential risks and complications [25].
In our study, eight out of the 18 patients received primary radiation treatment for their disease and two of whom underwent additional irradiation after relapsing. Eventually, three patients suffered from complications due to radiotherapy (radio-necrosis in two and oro-cutaneous fistula in one). It appears to be very risky to apply radiation to wounds contaminated with cancer cells through the skin or mucosa.
Therefore, PTS could be a very good alternative treatment when patients with incurable HNC have previously had full-dose radiotherapy, the tumor seems to be unresponsive to radiotherapy, or the patient had cancer-related wound problems. One desired outcome of PTS is to reduce the size of the mass, since large masses, such as unresectable laryngopharyngeal tumors, cause obstructive speech, swallowing, and breathing. Tumor debulking and reconstruction could be also valuable for exophytic neck/cutaneous masses, with minimal surgical morbidity [8]. Although the survival rate might not improve, surgical management of foul odor, pain, bleeding, and infection associated with skin wound problems has the potentialto improve patient quality of life [30]. One study presented the outcomes of surgical interventions for symptoms arising from advanced HNC, and it included debridement and debulking, mandibulectomy, maxillectomy, the use of free flap reconstruction and major vessel ligation [9]. The authors suggested that surgical palliation can be performed safely while achieving symptom relief in a highly selected group of patients. Similarly, half of the patients in our series experienced complete pain relief after PTS and most of the wound problems were resolved, leading to improved quality of life in these patients.
Another question in the PTS is how long PTS is effective in the management of symptom in patients with incurable HNC. It is hard to draw any generalized conclusion from our series; however, the remaining tumor seems to re-grow at post-operative 1 to 2 months with an intact skin (without wound problems) (Fig. 4). Thus, PTS should be followed by an adequate reconstruction procedure notto delay surgical wound healing over 1 month, and the additional cancer treatment within 2 months after PTS appears to be appropriate.
Some limitations of this study include its retrospective descriptive nature and the lack of evaluation tools to assess symptoms and response to PTS. Moreover,the number of patients included in this study was too small to draw definite conclusions. In addition, differences among the patients regarding symptoms, extent of tumors and performance status made it difficult to set common surgical indications for PTS. Therefore, it is essential to determine an individualized PTS plan through accurate evaluation, multidisciplinary cooperation, and patient consultation. Of particular note, successive treatments after PTS such as radiotherapy, chemotherapy or targeted molecular therapy could be applied in patients who had undergone supportive care only. This finding suggests the possibility of improving patient survival. However, large prospective comparative studies are needed to validate our preliminary results.
In conclusion, PTS could provide a meaningful benefit to selected patients with incurable HNC, in terms of pain control and cancer wound management. In addition, PTS could provide an opportunity for the subsequent treatment for some patients who were initially not amenable to the further treatment. Thus, PTS is a considerable option for selected HNC patients, based on the accurate evaluation of tumor extent, multi-disciplinary consultation, and patient counseling.