INTRODUCTION
Gastric cancer is a highly heterogeneous disease, the fifth most common cancer, and the fourth leading cause of cancer deaths worldwide. More than one million new diagnoses are confirmed, and an estimated 769,000 patients died from gastric cancer in 2020 [1]. The poor prognosis of gastric cancer has gradually improved over time, but remains at a low level, despite advances in understanding the disease [2]. The prognosis of gastric cancer can be determined according to several conditions, and various attempts to predict the survival of gastric cancer have provided grounds for establishing standard treatment guidelines for gastric cancer, including targeted therapy.
The American Joint Committee on Cancer (AJCC) [3] recommends staging as the best prognosis predictor for all cancer types, including gastric cancer. Several recent studies have also sought to base prognosis predictions on other factors, including histologic type and grade, microsatellite instability (MSI) status, age at diagnosis, gender, race, primary tumor location, previous treatment modality, and some biomarkers, including overexpression of human epidermal growth factor receptor 2 (HER2) [4], mesenchymal epithelial transition (MET) [5], and epidermal growth factor receptor [6]. Depending on the stage, surgery is performed in stage I to III, and postoperative adjuvant treatment can be performed for gastric cancer corresponding to stage II and III. In stage IV, based on the presence or absence of the HER2 target, patients receive HER2 targeted therapy or immune checkpoint blockers in addition to palliative systemic chemotherapy.
As with other cancers, complete surgical resection is the most effective treatment option; however, gastric cancer is often diagnosed only at an advanced stage, except in Japan and South Korea, where population screening is widely practiced. Recurrence occurred within 2 years in about 80% of gastric cancers, and 86.9% of the recurred cases had distant metastases [7].
For resectable recurrent gastric cancer occurring after surgery, only medically fit patients can receive local therapy such as re-operation or concurrent chemoradiation therapy. In a way, palliative systemic therapy is almost the only treatment option for advanced unresectable recurrent gastric cancers. In a Cochrane review, chemotherapy provided a survival benefit of 6.7 months compared to supportive care [8]. It is common practice for patients who can tolerate chemotherapy to continue receiving chemotherapy because the survival benefit of salvage chemotherapy is also available in the 2nd line and more treatment [9].
Treatment based on the characteristics of an individual patient’s disease is essential because it allows more precision in the recommended therapy and a better understanding of the ultimate prognosis. Targetable drugs like trastuzumab or nivolumab are currently being used for HER2 and MSI cancer types, which will allow personalized treatment. The reliability of study results is also increased by balanced matching of both groups and subgroup analysis and stratification in randomized clinical trials. Therefore, studies to find factors associated with survival are a preferred topic in cancer research.
Studies of other de novo or recurrent metastatic cancers (breast, lung, and colorectal) have found that the type of disease determines the prognosis and survival outcome [10-15]. To our knowledge, no literature has been published comparing the prognoses of de novo metastatic and recurrent metastatic disease in gastric cancer. In this study, our objective was to evaluate the prognostic impact of recurrent versus de novo cancer in gastric cancer patients who received a new diagnosis between 2012 and early 2022. In this study, we will describe and compare the two groups based on clinical characteristics, patient demographics, treatment, and survival outcomes.
METHODS
Study population
We reviewed all patients with pathologically confirmed gastric cancer who were diagnosed between January 2012 to June 2022 at Samsung Changwon Hospital, and only patients who had received palliative chemotherapy for at least 30 days were eligible to participate in the study. We chose 2012 because it is the year Korea approved trastuzumab for reimbursement as a palliative first-line chemotherapy treatment for gastric cancer.
The de novo cohort was defined as patients who presented with stage IV disease at the time of gastric cancer diagnosis. The recurrent cohort included patients with stage I to III gastric cancer who relapsed with metastatic disease after initially undergoing a gastrectomy or curative therapy via endoscopy. We used the AJCC eighth edition to stage the cases. Patients who died within 30 days after palliative chemotherapy, were lost to follow-up after diagnosis, or had other malignancies were excluded from the analysis.
Outcomes and variables
Two registered nurses who were not directly related to patient treatment independently collected data on patient demographics, clinical course, pathological findings, treatment, and survival outcomes from electronic medical records. We obtained age, gender, performance status (Eastern Cooperative Oncology Group [ECOG]), height, weight, smoking history, HER2 status, metastasis sites, and curative treatment type in the recurrent cohort at the time of metastasis in both groups, and we collected tissue type and differentiation from the pathologic report at initial diagnosis of gastric cancer. Chemotherapy details and date of death or recurrent metastasis were collected based on the patient’s last follow-up date.
The primary purpose of this study was to compare the overall survival (OS) of de novo and recurrent metastatic disease in gastric cancer. OS was defined as the time from the date of metastasis to death, and the date of recurrent metastasis was defined as the date identified by pathologic or imaging confirmation. Further objectives included (1) the comparison of post-distant recurrence survival (PDRS) of patients and the metastasis-free interval (MFI) in the recurrent metastatic cohort; (2) a comparison of survival time according to the variables in each group of the de novo and recurrent cohorts; (3) association between those variables and survival; and (4) median survival according to the chemotherapy regimens after metastatic disease. PDRS was defined as the time from the date of metastatic recurrence to death, and MFI was defined as the time from initial curative treatment to metastatic recurrence.
Statistical analysis
We applied multivariable Cox proportional regression to evaluate the association between the disease cohorts and survival, controlling for factors associated with OS in the univariate analysis at a level of significance of P=0.1. The model was adjusted for potential confounding variables, including age, performance status, body mass index, smoking history, tumor location, surgery type, HER2 status, degree of differentiation, and type of gastric cancer based on histology. An independent t-test was used to evaluate the significance of the mean differences between the continuous variables. Outcome survival was estimated using the Kaplan-Meier survival analysis and compared across groups using the log-rank test. Patients who were alive when the data were analyzed were censored at the time of the last available follow-up. A P-value of < 0.05 was considered statistically significant. The association of PDRS and MFI is shown in a scatter plot. All statistical analysis was performed using Stata version 14.0 software (Stata Corp.).
Statement of ethics
The study was conducted in accordance with the World Medical Association Declaration of Helsinki and the study protocol was reviewed and approved by the Institutional Review Board at Samsung Changwon Hospital (IRB No. SCMC 2022-07-008). The Institutional Review Board also approved and issued a waiver of informed consent for our retrospective study.
RESULTS
The de novo metastatic cohort included 167 patients with a mean age of 68.15±12.00, with 123 (73.6%) males and 44 (26.4%) females. The recurrent metastatic cohort included 112 patients with a mean age of 65.67± 12.13, with 74 (66.1%) males and 38 (33.9%) females. Table 1 shows patient characteristics categorized by de novo and recurrent cohorts. Compared to the recurrent cohort, the de novo cohort had a shorter duration of palliative chemotherapy and more patients with low body mass index. Age, gender, performance status, smoking history, primary tumor location, and pathologic features, including HER2 expression, were statistically balanced between the two cohorts.
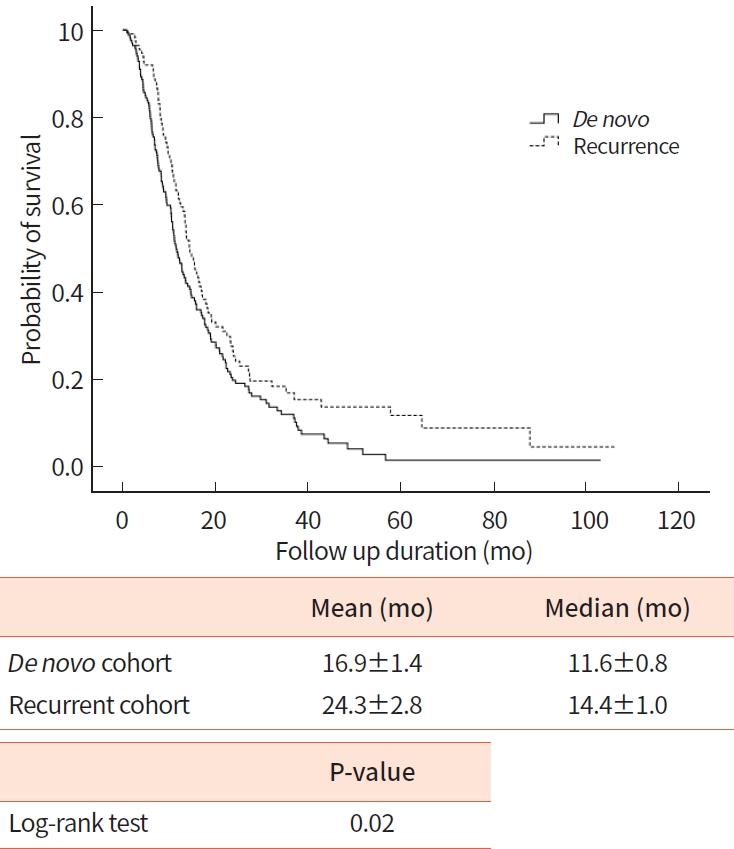
The comparison of survival between the two groups, which is the main objective of this study, showed a significantly longer duration in the recurrent cohort compared to the de novo cohort (median survival of 11.6± 0.8 months vs. 14.4± 1.0 months, P=0.02) (Fig. 1).
In the survival analysis based on treatment with a specific anticancer regimen, the survival times are ranked from longest to shortest for these standard gastric cancer chemotherapies: platinum, taxane, irinotecan, immune checkpoint inhibitor, and fluoropyrimidine (Table 2). The difference in survival between the two cohorts according to the type of regimen was significant in the group receiving the platinum-based chemotherapy, which is mainly used as a first-line treatment for gastric cancer.
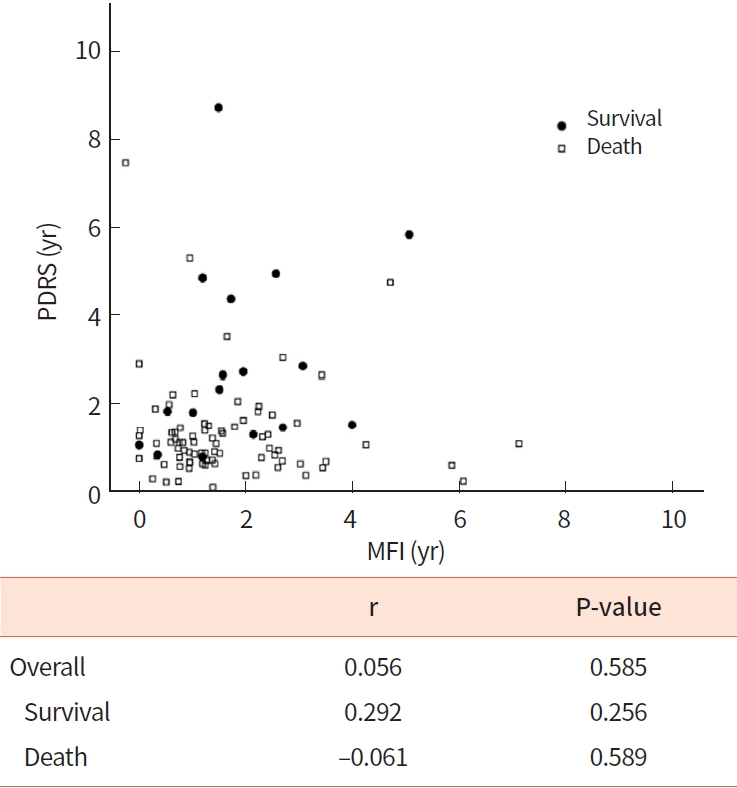
The survival of both cohorts showed no significant differences in most subgroups. Still, a significantly longer survival was observed in the recurrent cohort when the site of the metastasis was the peritoneum (Table 3). In the multivariate analysis of variables, the prognosis was relatively poor in patients aged 70 years or older (relative risk [RR], 1.71; P=0.018), and the RR was significantly higher in the subgroup including mucinous and signet ring cell differentiation (RR, 1.97; P=0.035 than in the well, moderately, or poorly differentiated subgroups) (Table 4). The PDRS according to MFI, an analysis limited to the recurrent metastatic cohort, was not statistically significant, but positive correlations were observed in the survivors and negative correlations in the deceased (Fig. 2).
DISCUSSION
This cohort study provides a rare opportunity to compare survival and clinical outcomes for patients with de novo or recurrent metastatic gastric cancer in a real-world population. More importantly, we found that de novo metastatic gastric cancer patients had significantly worse survival outcomes than the recurrent group (11.6 months vs. 14.4 months, respectively; P =0.02), even after adjusting for other variables (hazard ratio [HR], 1.38). There might be a difference in survival between the de novo and recurrent metastatic diseases, but these findings strongly suggest that more research is needed.
Studies can determine future treatment options by identifying the most effective treatments for each patient. In research, it is crucial to classify cancer groups based on the factors that impact prognosis, and studies are often based on characteristics such as anatomy, pathology, demography, and molecular biology. In gastric cancers, there have been few studies that classified patients by metastatic disease type, although classifications have been used such as anatomy (cardia and non-cardia), pathology (adenocarcinoma and non-adenocarcinoma), demography (Asian and non-Asian), and molecular biology (CpG island methylator phenotype [CIMP], Epstein-Barr virus [EBV], microsatellite instability [MSI], genomically stable [GS]). Survival of other cancers has been studied by comparing the classifications of de novo and recurrent disease according to the metastatic disease type. Breast cancer studies have frequently compared de novo disease and recurrent disease, and the survival of patients with de novo disease is superior to those with recurrent disease [11,12,16]. However, retrospective lung cancer studies have found the survival outcomes of recurrent disease superior to those in de novo disease [10,13,14].
In East Asian countries (China, Japan, and South Korea), gastric cancer patients commonly receive endoscopic screening followed by gastrectomy. Endoscopic screening is not a common practice in other countries, so early diagnosis is not easy and there is a high rate of distant metastasis when gastric cancer is diagnosed. Because of this low rate of recurrent gastric cancer, there may be few studies comparing the survival of de novo and recurrent disease in gastric cancer.
The VIKTORY umbrella study was one of the most extensive studies that classified patients based on clinical sequencing of metastatic gastric cancer, comparing the survival of de novo and recurrent disease through Cox regression analysis [17]. The study included 557 patients (80.7%) with de novo disease and 138 patients (19.3%) with recurrent disease and found a longer survival time in the recurrent disease group (HR, 0.77) than in the de novo group, although the results were not statistically significant. Our study and the VIKTORY study both show that longer survival rates occurred in patients with recurrent rather than de novo disease, similar to what was found in studies of lung cancers.
Although the reasons for the difference in survival between gastric cancer patients with de novo and those with recurrent gastric distribution are unknown, we are exploring several explanations. Our study is retrospective, and the intrinsic differences between the groups could create an unbalanced distribution, including differences in molecular biology. The results could be affected by selection bias, but the population characteristics of our study are close to the actual clinical practice. The median age of our study’s patient population was 68.2 years old in the de novo cohort and 65.7 years old in the recurrent cohort, suggesting that the real-world data are closer to the Surveillance, Epidemiology, and End Results (SEER) data (68 years old) [18] than the results (56 to 62 years) of previous significant randomized phase III studies in palliative setting (ToGA, Checkmate 649) [19,20].
The use of adjuvant chemotherapy before metastatic relapse in recurrent disease is another possible explanation for the survival difference, as was the case in several lung cancer studies that showed that adjuvant chemotherapy had a beneficial effect on post-recurrence survival [14,21,22]. Use of gastrectomy could also be an important factor; a large-scale retrospective study on palliative and curative chemotherapy in gastric cancer showed that patients with a previous gastrectomy had a more favorable prognosis, no matter which course of chemotherapy they received [23]. We propose that gastrectomy reduces tumor burden and prevents complications such as tumor bleeding, perforation, and obstruction.
The method of gastrectomy could also affect survival, with a recent meta-analysis showing that subtotal gastrectomy had a significantly better 5-year survival outcome than total gastrectomy (TG) [24]. The type of surgery used to remove the primary tumor may influence the prognosis; TG is a more invasive procedure, which could also affect long-term survival. Our study also showed an unfavorable trend for survival in the TG group, although the number was not significant (HR, 1.13; 95% confidence interval, 0.73 to 1.76; P=0.585). In addition to the risk depending on the surgery type, the location of the primary tumor can affect prognosis. Colorectal cancer that occurs in the same gastrointestinal tract, shows markedly different characteristics and survival of distal and proximal colons [25]. Distal and proximal colons were embryologically different and molecular heterogeneous. So, it’s the same large intestine, but made to look like different organ in some respects. There are differences between tumors arising from the distal antrum and the proximal fundus of gastric cancer, which is consistent with the TCGA data [26]. Chromosomal instability (CIN) type was common in proximal tumor, and MSI and GS types were relatively common in distal tumor. The authors reported that relapse was relatively common in the CIN type found at high frequency in proximal tumors, which is consistent with the high rate of proximal cancer in the recurrent metastatic group in our study.
Our study showed that patients with recurrent metastatic disease with peritoneum involvement were more likely to survive than de novo patients. Because it does not always present with measurable lesions, peritoneal metastatic carcinoma is hard to diagnose with radiologic testing; this form of cancer presents instead with ambiguous clinical findings like ascites or hydronephrosis. Difficulty in tissue collection from the peritoneum makes cancer at this site harder to diagnose, even if suspected. Because of these factors, patients with previous peritoneal metastasis receive better surveillance of this area than de novo patients. Routine surveillance could make the calculation of survival time in recurrent disease seem longer because the diagnosis was made earlier, regardless of whether the patient lived longer.
Another important factor affecting survival is the MFI: the recurrent group has a longer survival time when the MFI is long. In comparison, a shorter disease-free interval (DFI) is shown in breast cancer studies to mean a more significant gap in survival outcome between the de novo and recurrent groups; the survival time between both groups is gradually reduced as the DFI increases [27-29]. Survival rates between the two cohorts differed only in the patients who used a platinum-based regimen (Table 2).
In the recurrent disease group, a number of the patients were treated with capecitabine plus cisplatin as adjuvant chemotherapy, and their MFI was at least 1 year. However, patients with recurrent malignancies might not have received the platinum-based palliative treatment because of their poor health, or they might have had a cancer recurrence within 6 months (a platinum refractory state); in these cases, the platinum agent would not be used. Our study showed that patients treated with palliative platinum chemotherapy had favorable survival rates, as they included patients with long MFI.
To conclude, our real-world cohort study is the first to show the survival and characteristics of recurrent metastatic gastric cancer, which accounts for 20% to 25% of stage IV gastric cancer patients. The prognosis of patients with recurrent metastatic gastric cancer was significantly better than those with de novo disease. Future systematic and large-scale cohort studies are needed to confirm our findings.