INTRODUCTION
Adrenalectomy is the treatment of choice for sporadic unilateral adrenal tumors [1]. However, adrenal function cannot be preserved in the case of bilateral adrenal tumors. Accordingly, tumorectomy or hemiadrenalectomy is frequently recommended in patients with a history of unilateral adrenalectomy, to avoid adrenal insufficiency. Such cases occur in patients with hereditary pheochromocytomas associated with von Hippel-Lindau (VHL) disease or in multiple endocrine neoplasias [2].
Thermal ablation has been established as an alternative treatment for patients who are poor surgical candidates owing to a higher risk of postoperative morbidity or mortality. This minimally invasive treatment contributes to the preservation of adrenal function and the removal of adrenal tumors. A percutaneously accessible route is key to achieving successful ablation. Because the adrenal gland is surrounded by many critical organs such as the liver, spleen, kidney, gastrointestinal tract, pancreas, diaphragm, and major vessels, it is not always possible to approach adrenal tumors. The only safe and accessible pathway for adrenal biopsy or ablation is the trans-hepatic route to approach a right adrenal tumor to avoid lung injury [3-5]. To the best of our knowledge, there have been no reports on renal ablation procedures for adrenal tumors.
The purpose of this case report was to show our experience of computed tomography (CT)-guided trans-renal radiofrequency ablation (RFA) and hydrodissection for a recurrent pheochromocytoma in a patient with VHL disease.
CASE REPORT
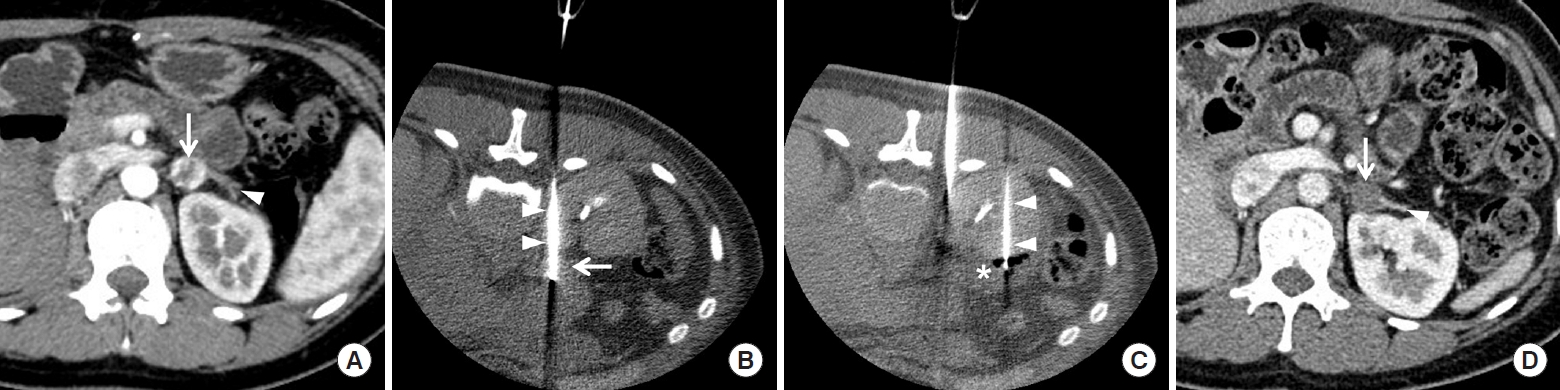
A 35-year-old woman was transferred to our hospital for treatment of recurrent pheochromocytoma. She had been diagnosed with VHL disease 10 years previously and undergone right adrenalectomy and left hemiadrenalectomy for recurrent pheochromocytoma. Recently, the patient presented with elevated levels of catecholamines in the urine and plasma; contrast-enhanced CT showed a recurrent pheochromocytoma in the residual left adrenal gland. Her endocrine clinician recommended adrenalectomy but decided to perform RFA to preserve adrenal function. Pre-ablation CT showed a small pheochromocytoma located in the medial portion of the residual left gland (Fig. 1A). The tumor measured 1.5 cm, was strongly enhanced, and was surrounded by the left kidney, jejunum, spleen, pancreas, diaphragm, and aorta.
An interventional radiologist, with 10 years of experience in percutaneous thermal ablation, introduced a 17-gauge RFA electrode (Proteus, STARmed) through the left renal parenchyma under CT guidance (Fig. 1B). Blood pressure was stable, including during tumor targeting by the electrode. A 20-gauge Chiba needle was introduced through the left renal parenchyma for hydrodissection (Fig. 1C). A total of 400 mL 5% dextrose water was intermittently instilled to displace the jejunum and pancreas from the pheochromocytoma. Blood pressure increased rapidly, suggesting a hypertensive crisis, immediately after the first ablation cycle; thus, beta- and alpha-blockers were intravenously injected to control blood pressure. When the radiofrequency (RF) electrode was withdrawn, the renal parenchyma was cauterized for approximately 20 seconds to minimize renal bleeding. The tumor was completely ablated without heat damage to the neighboring organs. The patient was discharged without signs or symptoms of adrenal insufficiency. The levels of urine and plasma catecholamines normalized post-RFA and follow-up CT showed no signs of residual or recurrent pheochromocytoma (Fig. 1D).
Approval of Institutional Review Board or informed consent was not necessary because of case report.
DISCUSSION
Trans-renal ablation and hydrodissection were technically successful in the present case without significant complications. The kidney is a hypervascular organ compared with other critical organs. Therefore, non-vascular interventions are rarely performed through the renal parenchyma; thus, there are few reports on trans-renal ablation procedures in the literature for treating adrenal tumors that are not percutaneously accessible. Additionally, trans-renal hydrodissection is a rare interventional procedure to displace neighboring organs from the adrenal tumor. The left adrenal gland is surrounded by several critical organs such as the kidney, spleen, pancreas, aorta, duodenum, jejunum, stomach, diaphragm, and lungs. Thus, mechanical or thermal injury to these organs should be avoided. Damage to the gastrointestinal tract during ablation can lead to serious complications, such as perforation, peritonitis, abscess, or sepsis [2,6]. An injured pancreas may develop acute pancreatitis, juice leakage, or abscess formation [7]. A perforated aorta can cause massive bleeding and sudden death [8]. An injured spleen may induce bleeding, which may be exacerbated if the splenic vessels are injured [9]. If the diaphragm is injured, various complications may occur such as chest pain, dyspnea, eventuation, or hernia [10]. Injured lungs may result in pneumonia, effusion, fistulas, or pneumothorax [2,6].
The adrenal gland is frequently located close to the anterior aspect of the upper pole of the kidney. If an RF electrode is introduced in a perpendicular direction from the back, it should pass through the renal parenchyma to target the adrenal tumor. A 17-gauge RF electrode may result in renal bleeding; however, electrocauterization may help reduce the amount of bleeding during electrode withdrawal. Trans-hepatic approaches are frequently used to target right adrenal tumors to avoid mechanical or thermal injury to other organs [3-5]. However, this technique cannot be applied to target left adrenal tumors; thus, in the present case, a trans-renal procedure had to be employed.
Pheochromocytomas tend to be recurrent and multifocal in patients with VHL disease. The treatment of choice is adrenalectomy, which results in adrenal insufficiency if bilateral. Therefore, thermal ablation can be used as an alternative treatment to increase steroid-free survival rates. Adrenal insufficiency typically occurs when more than 80% of the adrenal glands are destroyed. A multidisciplinary discussion is necessary among endocrinologists, surgeons, and radiologists in each case, to determine the appropriate treatment modality for patients with pheochromocytomas [2,6].
Trans-renal ablation procedures present several limitations. First, these ablation procedures are difficult to master; thus, an expert in these approaches is required to increase the chance of efficient tumor ablation. Careless manipulation of the electrode may increase bleeding during the procedure, leading to transfusion or embolization. Second, pre-ablation planning needs to be carefully performed to determine whether a trans-renal procedure is necessary. CT fluoroscopy helps interventional radiologists to precisely target adrenal tumors via the renal parenchyma. Third, premedication with beta- and alpha-blockers is necessary to reduce the likelihood of a hypertensive crisis [2,6]. These antihypertensive agents should be administered intravenously, immediately after blood pressure is elevated.
In conclusion, trans-renal ablation procedures can be invasive and should be carefully performed by an expert, in cases where this approaching route is the only option to reach the adrenal tumor. Minimizing manipulation and precise targeting are key techniques for achieving successful adrenal ablation without significant complications.