INTRODUCTION
Central nervous system (CNS) metastases, including brain and leptomeningeal metastases, in non-small cell lung cancer (NSCLC) patients are one of the main reasons leading to disease-related death and can cause significant impairments in the quality of life. More than half of NSCLC patients with epidermal growth factor receptor (EGFR) mutation exhibit CNS metastases during the treatment course [1]. The available treatments for parenchymal CNS metastasis are limited to localized therapies such as whole brain ra diation therapy or stereotactic radiation surgery; however, these approaches have shown unsatisfactory survival benefit [1]. The treatment of leptomeningeal metastases, including intrathecal chemotherapy, also remained challenging due to difficulties in efficiently applying the drug and treatment related toxicities [1]. Systemic cytotoxic chemotherapy has been considered for CNS metastases, but little benefit has been observed because of the poor penetration of drugs across the blood-brain barrier (BBB) [1,2].
With the development of EGFR targeting agents, research on developing therapeutic strategies for CNS metastases has focused on how to maintain therapeutic drug concentrations in cerebrospinal fluid (CSF). Tyrosine kinase inhibitors (TKIs) have been recently designed to increase BBB penetration and also avoid efflux. One of the well-known mechanisms underlying poor drug concentration in the CSF is related to P-glycoprotein (multidrug resistance protein 1 [MDR1]) or breast cancer resistance protein (BCRP)-mediated efflux [3]. The 3rd generation EGFR TKIs osimertinib and lazertinib are representative examples of molecules that are not as affected by efflux transporters, which increased the relative exposure of intracranial tumor and plasma ratio compared with 1st and 2nd generation EGFR TKIs [3,4]. High concentration of drugs in intracranial tumors demonstrated clinically significant benefits in both preventing and treating CNS lesions in patients with EGFR-mutated tumors [5-7].
AZD3759 (zorifertinib) is a novel EGFR TKI that was designed to not bind MDR1 and BCRP to avoid efflux transport; it shows a much higher unbound brain to unbound blood ratio (Kpuu, brain) and unbound brain to unbound CSF ratio (Kpuu, CSF) compared with EGFR TKIs including gefitinib, erlotinib and afatinib, enabling AZD3759 to maintain a sufficient drug therapeutic concentration in the CSF [2,8]. In the BLOOM phase 1 clinical trial on the activity and safety of AZD3759 in EGFR-mutant NSCLC with CNS metastasis, clinical benefit in both CNS lesions (objective response rate [ORR], 83%) and extracranial disease (ORR, 72%) was observed [9]. Additionally, a phase 3 clinical trial of AZD3759 for first-line treatment for EGFR-mutated NSCLC with CNS metastasis reported that AZD3759 was more favorable than the first-generation EGFR TKIs, gefitinib and erlotinib; the median progression-free survival (PFS) of these two treatments was 15.2 and 8.3 months, respectively [10].
In this case report, we report a patient with EGFR-mutated NSCLC who was initially diagnosed with CNS metastases and treated with AZD3759 as a part of the BLOOM study.
CASE REPORT
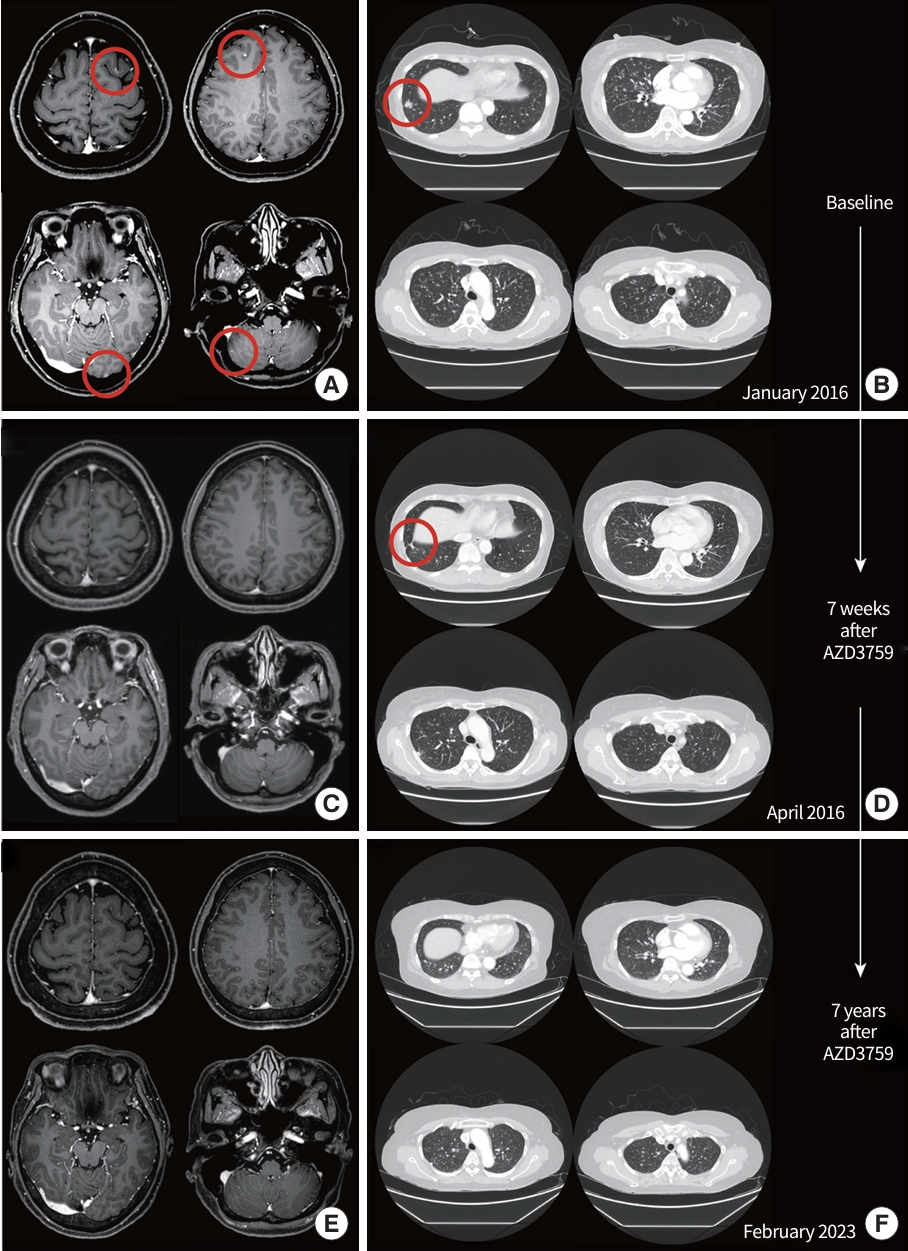
A 53-year-old, female never-smoker patient presented with an abnormal chest X-ray showing multiple scattered nodules at both lungs during a routine health screening. Chest computed tomography (CT) showed a 17 mm sized nodule at the right lower lobe, and miliary metastatic nodules were observed in both lungs. Brain magnetic resonance imaging presented multiple tiny metastatic nodules in both cerebral hemispheres and the right cerebellum without leptomeningeal metastases (Fig. 1A, B). Other than the aforementioned lesion, no metastatic lesion was observed in the abdomen and pelvis CT, positron emission tomography CT scan taken before the treatment. CSF analysis showed no neoplastic cells.
Video-assisted thoracoscopic wedge resection of the right upper lobe and right lower lobe was performed on January 2016, to confirm the histological composition, and adenocarcinoma with moderate differentiation was confirmed. EGFR exon 19 deletion was identified using real-time polymerase chain reaction assay; no other molecular alteration was observed. From the initial staging workup showing stage IV, cT1N0M1 (by the American Joint Committee on Cancer 8th edition of the tumor, node, metastasis [TNM] classification), systemic treatment was planned.
As an initial treatment, the patient was enrolled in the BLOOM study and received AZD3759 on March 2016, 300 mg dose orally twice a day, as a first-line agent. After 3 weeks of treatment, the patient reported grade 2 skin toxicity, including dry skin and pruritus, which led to the discontinuation of AZD3759 for 1 week and the application of oral minocycline and topical steroids. After the appropriate supportive care for 1 week, symptoms improved to less than grade 1, and AZD3759 was resumed at a reduced dosage of 200 mg twice a day. The first image evaluation was taken after 7 weeks of AZD3759. Complete response was observed in brain metastatic lesions, and miliary metastatic nodules at both lungs showed a decrease in both size and number (Fig. 1C, D).
During the treatment course, two subsequent dose reductions were performed because of skin toxicities. At 5 months after treatment initiation, October 2016, the dosage was reduced to 150 mg twice a day because of grade 3 pruritus. After 3 years of treatment, in February 2019, the dosage was once again reduced to 100 mg twice a day because of grade 2 scalp rash. Both of the events were well managed with supportive care after the dose reduction.
Until May 2023, the patient is still on the treatment, showing a sustained response with AZD3759 over 85 months without disease progression or additional toxicities (Fig. 1E, F).
Approval Institution Review of Board or informed consent was not neccessary because of case report.
DISCUSSION
This case exhibited an unprecedented response, showing the long duration of response to treatment for CNS metastases for over 7 years and which is still ongoing. Our results are concordant with the outcomes observed in prior pre-clinical studies of AZD3759. In a pre-clinical study using a mouse model, AZD3759 showed superiority in penetration of CNS and antitumoral activity for EGFR-mutated NSCLC. The median Kpuu,brain and Kpuu,CSF of AZD3759 were 0.65 and 0.42, respectively, and AZD3759 showed a higher CNS penetration compared with erlotinib (0.13 and 0.14, respectively) [8]. This outcome has been also reproduced in the clinical setting showing CNS efficacy of AZD3759 in phase 1 and 2 trials [2,8,9,11]. A randomized phase 3 trial investigating AZD3759 (200 mg twice a day) as the first-line treatment for EGFR-mutant NSCLC with untreated CNS metastasis demonstrated superior systemic and intracranial antitumor efficacy compared with first-generation EGFR TKIs (gefitinib or erlotinib) [10]. The intracranial median PFS and confirmed ORR for AZD3759 were 15.2 months (95% confidence interval [CI], 12.5 to 19.4) and 75.0%, respectively; the median duration of response was 13.8 months (95% CI, 8.5 to 22.1). Considering that approximately 8% of the cases showed leptomeningeal metastases, these numbers were comparable to the results shown with 3rd generation EGFR TKIs, which showed high BBB penetration profiles in pre-clinical studies and better clinical efficacy in CNS metastasis in randomized phase 3 studies. In a subgroup analysis in the FLAURA study, osimertinib showed an ORR of 66% in patients with measurable and/or nonmeasurable CNS lesions [12]. In the LASER 301 study, lazertinib demonstrated a median PFS of 16.4 months in patients with brain metastases [6]. This outcome is in line with our results, showing a durable CNS response, which may be attributed to the underlying pharmacokinetic properties of AZD3759 and its ability to penetrate the BBB [9].
In the current case, the patient was initiated on a dosage (300 mg twice a day) that was higher than the dosage in the phase III trial (200 mg twice a day), and eventually underwent dose reduction. Nevertheless, we observed persistent clinical benefits at a reduced dosage (100 mg twice a day). There is early clinical evidence from the dose-escalation phase of the BLOOM study that showed that AZD3759 was effective in both intracranial and extracranial lesions, even with a lower dosage than the currently recommended dose [9]. Among the four patients in the 100 mg twice daily cohort who had assessable CNS target lesions, two patients showed partial response and one patient showed stable disease as the best response, which suggests the possibility of persistent response with the reduced dose for patients who experience toxicity to 200 mg twice a day as in the current case.
In conclusion, we observed a notable case of long-lasting efficacy for AZD3759 treatment against CNS and extracranial lesions, with no issue in long-term safety.