INTRODUCTION
Pneumonia refers to lung inflammation caused by bacterial or viral infection and pathologically to the condition where the alveolar spaces are filled with pus and the lungs become solid. The inflammation may affect the both lungs, one lung or only the certain lobe(s).
The pneumonia can occur in young and healthy people, but the condition is most dangerous for elderly people, infants, and patients with other disease(s), and those (immunocompromised patients) with impaired immune systems. Pneumonia affects approximately 450 million people globally (7% of the population) and results in about 4 million deaths per year [1]. It occurs about five times more frequently in the developing countries than in the developed countries. Viral pneumonia accounts for about 200 million cases. In the United States, approximately one million people are treated in the hospital for pneumonia in each year, and about 50 thousand people die of the disease. The disease is the leading cause of death owing to infection in children < 5 years of age worldwide, and pneumonia and influenza together are ranked as the eighth leading cause of death in the United States [2].
The pneumonia start with symptoms similar to those of cold and flu, then a high fever, chills and cough, and sputum follow. Other symptoms include chest pain, tachycardia, nausea and vomiting, headache, muscle pain, confusion or delirium, or skin discoloration and cyanosis. These symptoms may vary depending on the type of pneumonia and other underlying conditions.
The clinical, morphologic, and pathologic findings have been well known. However, still it is difficult to make an accurate diagnosis of pneumonia particularly regarding causative organisms related to the morphologic pneumonia. Meanwhile, the incidence of chronic pneumonia is increasing as a manifestation of pneumonia in mild immunocompromised patients. The aim of this review was to update the information on pneumonia focused on imaging features and new antibiotic agent in the diagnosis and treatment of pneumonia in the era of personalized medicine.
Settings of pneumonia development
Community-acquired pneumonia
Community-acquired pneumonia (CAP) is acquired in the community, outside of health care facilities. Compared with healthcare-associated pneumonia (HCAP), it is less likely to involve multidrug-resistant bacteria. Although the latter are no longer rare in CAP, they are still less likely. The mortality of CAP in cases of outpatients is reported to be 1% to 5%, whereas that in CAP necessitating hospitalization is reported to be as high as 25% [3,4].
Hospital-acquired pneumonia (also called nosocomial pneumonia)
Hospital-acquired pneumonia (HAP) is acquired in a hospital, specifically, pneumonia that occurs 48 hours or more after admission, which was not incubating at the time of admission. It is likely to involve hospital-acquired infections, with higher risk of multidrug- or extensively drug-resistant pathogens. The HAP may contain HCAP and ventilator-associated pneumonia [5].
Incidence of pathogens
CAP in patients of <60 years of age and without comorbidity
Streptococcus pneumoniae, Mycoplasma pneumoniae, respiratory viruses, Hemophilus influenzae, Chlamydia pneumoniae, and Legionella species are the most frequent organisms involved [6].
CAP in patients of >60 years of age or with comorbidity
S. pneumoniae , respiratory viruses, H. influenzae , aerobic gram-negative bacilli, and Staphylococcus aureus are the most frequently involved organisms [7].
Incidence of pathogens in pneumonia requiring hospitalization
They are S. pneumoniae, H. influenzae, polymicrobial organisms, anerobic gram-negative bacilli, Leginella species, S. aureus, C. pneumoniae, and respiratory viruses.
Hospital-acquired pneumonia
Gram-negative organisms including Pseudomonas aeruginosa, enterobactor species, Klebsiella pneumoniae, Escherichia coli, and H. influenzae account for approximately 60% of involved organisms; gram-positive bacilli including S. aureus and S. pneumoniae are involved in about 20% of infection; and fungi are involved approximately in 5% of HAP.
CLASSIFICATION
Morphologic classification
Pulmonary infection can also be classified into several radiologic and pathologic patterns according to its morphologic features. The three most common patterns are lobar pneumonia, bronchopneumonia, and interstitial pneumonia. Less common forms of infection include cellular bronchiolitis, septic embolism, miliary infection, and lung abscess. Because less common forms of infectious condition shall be dealt with the subheading of mixed infection, the three most common patterns are described here.
Lobar pneumonia
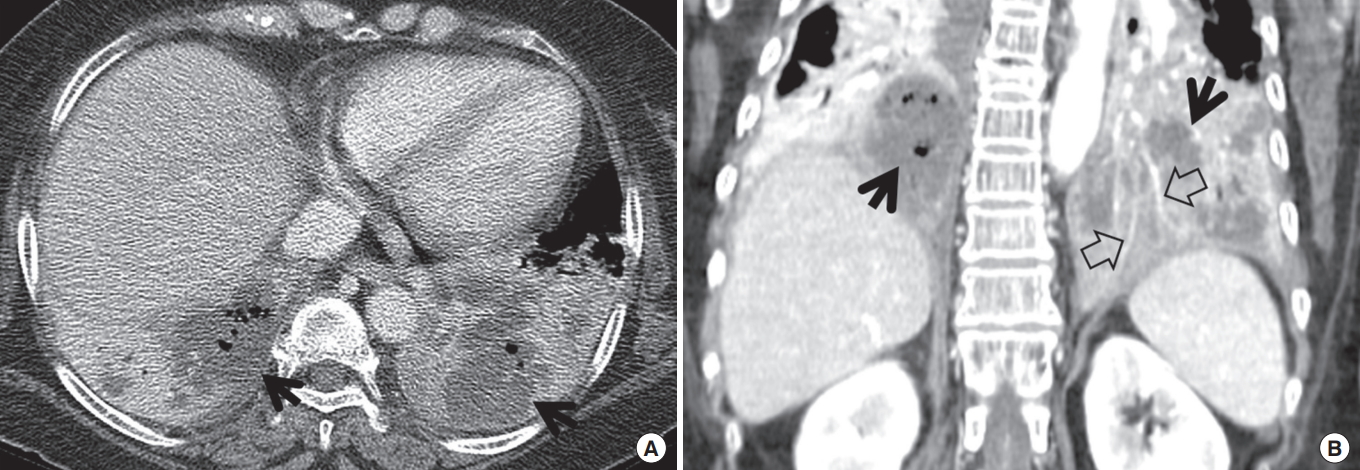
Lobar pneumonia is characterized histopathologically by filling of alveolar airspaces by an exudate of edema fluid and neutrophils. This filling is usually uniform within the affected lung and typically extends across pulmonary segments. The consolidation usually begins in the periphery of the lung adjacent to the visceral pleura, and spreads via interalveolar pores and small airways centripetally, sometimes to involve the entire lobe. Bronchi that remain filled with gas and become surrounded by the expanding inflammatory exudate are often seen as air bronchograms on computed tomography (CT) scans. The most common causative organisms are S. pneumoniae, K. pneumoniae (Fig. 1), and Legionella pneumophila.
On CT scans, homogeneous airspace consolidation involving adjacent segments of a lobe is the predominant finding. On high-resolution computed tomography (HRCT), areas of ground-glass opacities (GGOs) denoting incomplete filling of alveoli can be seen adjacent to the airspace consolidation (Fig. 1) [8]. The consolidation typically extends across lobular and segmental boundaries.
Segmental or lobar form of tuberculous pneumonia may occur in adults; in acquired immune deficiency syndrome (AIDS) or non-AIDS immunocompromised patients including pregnant women, elderly, diabetes, alcoholics, and transplanted patients. Multiple small cavities may be shown within the consolidative lesion [9,10].
Bronchopneumonia
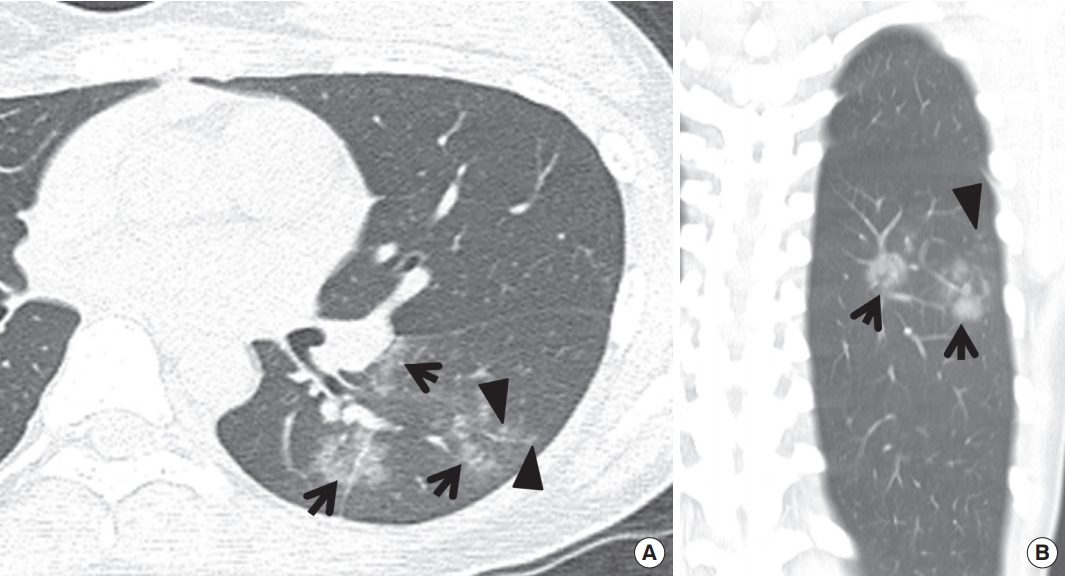
Bronchopneumonia is characterized pathologically by patchy, predominantly peribronchiolar inflammation. The reason why this localization is different from lobar pneumonia is unclear, but may be related to relatively less abundant edema formation (associated with more difficult spread of infection within the lung) and more virulent organisms (resulting in greater tissue destruction) in bronchopneumonia. Although initially patchy, progression of disease may result in lobular and segmental consolidation. The main causative organisms are S. aureus, H. influenzae, P. aeruginosa, and anaerobic bacteria.
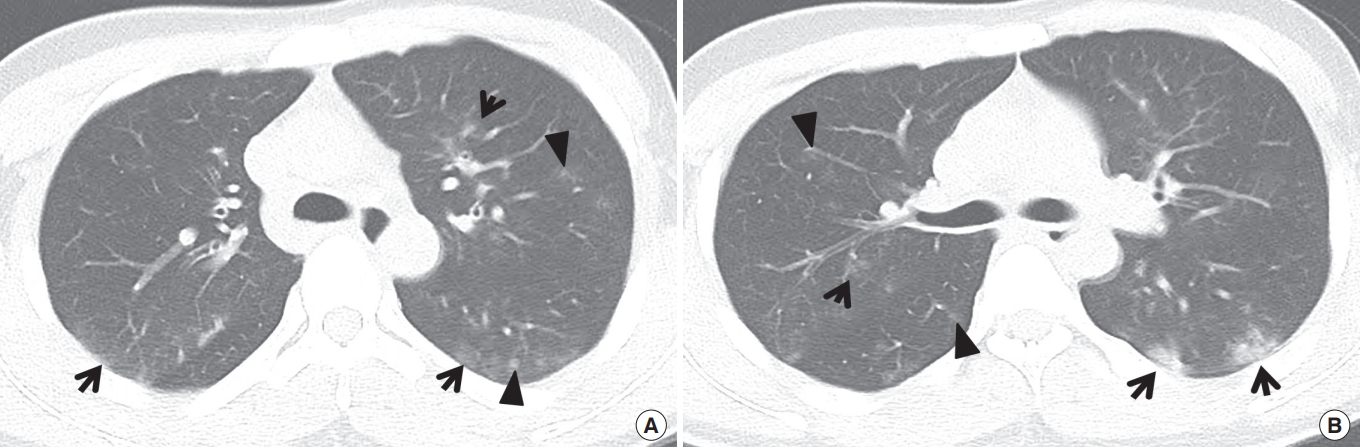
Characteristic findings on HRCT include centrilobular small nodules and branching nodular structures, airspace nodules, and multi-focal lobular consolidation or GGO (Figs. 2, 3) [8]. The small nodules and branching linear opacities result in an appearance resembling a tree-in-bud and are related to the presence of the inflammatory exudate in the lumen and walls of membranous and respiratory bronchioles and the lung parenchyma immediately adjacent to them. This appearance is similar to cellular bronchiolitis caused by viruses, M. pneumoniae and Chlamydia [8,11]. Unlike the latter (atypical pneumonias), however, the tree-in-bud pattern in bacterial bronchopneumonia usually comprises only a small proportion of the HRCT abnormalities. In addition, thickening of bronchovascular bundles is more frequently observed in atypical pneumonia, in which individual opacity tend to be distributed at the inner zone in addition to the middle and outer zones and be recognized smaller than those of bacterial pneumonias [8].
Pulmonary tuberculosis (TB) also presents with prototypical morphologic dense (much denser [Fig. 4] than ordinary bacterial pneumonia) bronchopneumonia. On CT, the lesion consists of tree-in-bud pattern, acinar nodule, lobular consolidation, and cavitating or noncavitating nodules or subsegmental or segmental consolidation. Bronchial wall thickening may be associated [9]. Clustering of tree-in-bud sign may result in CT-galaxy sign (Fig. 4).
Interstitial pneumonia
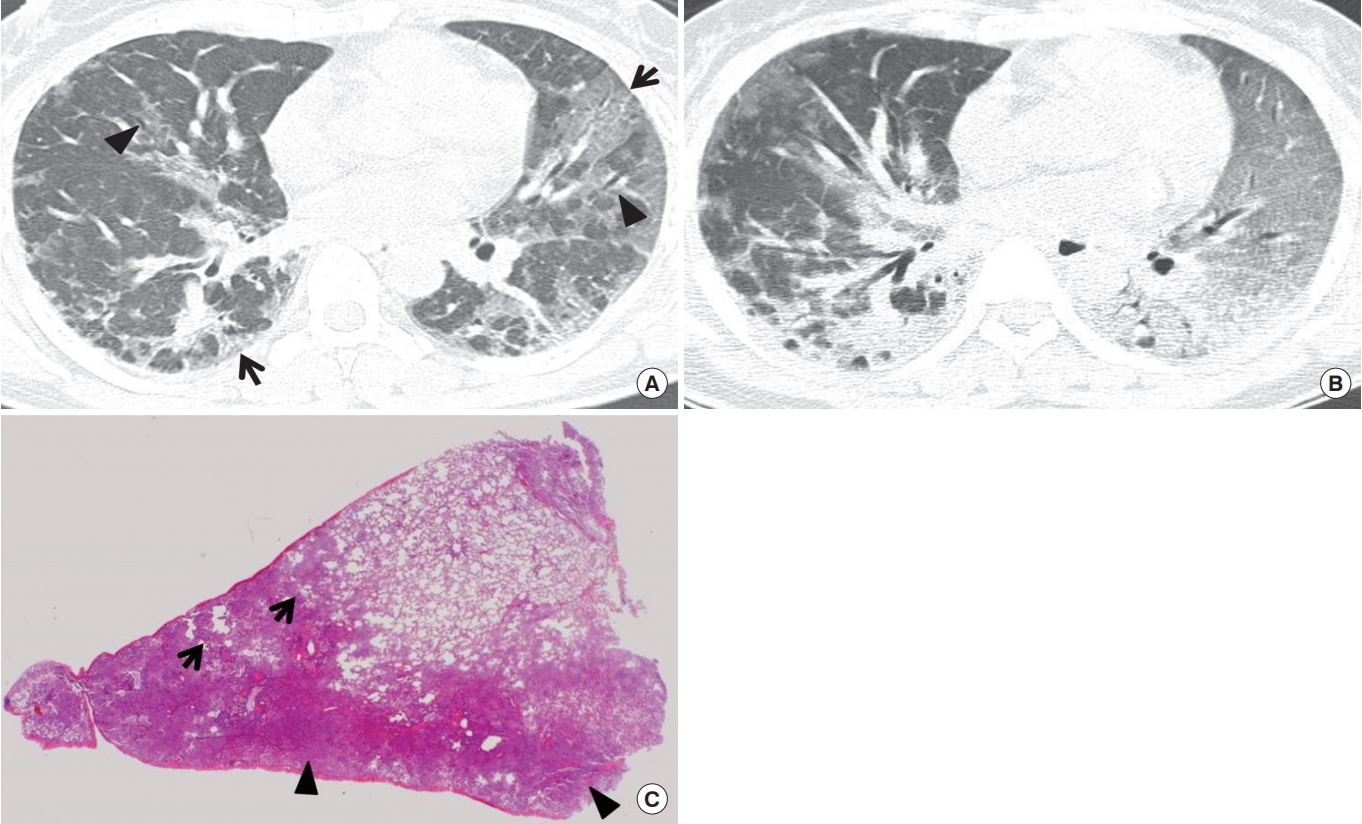
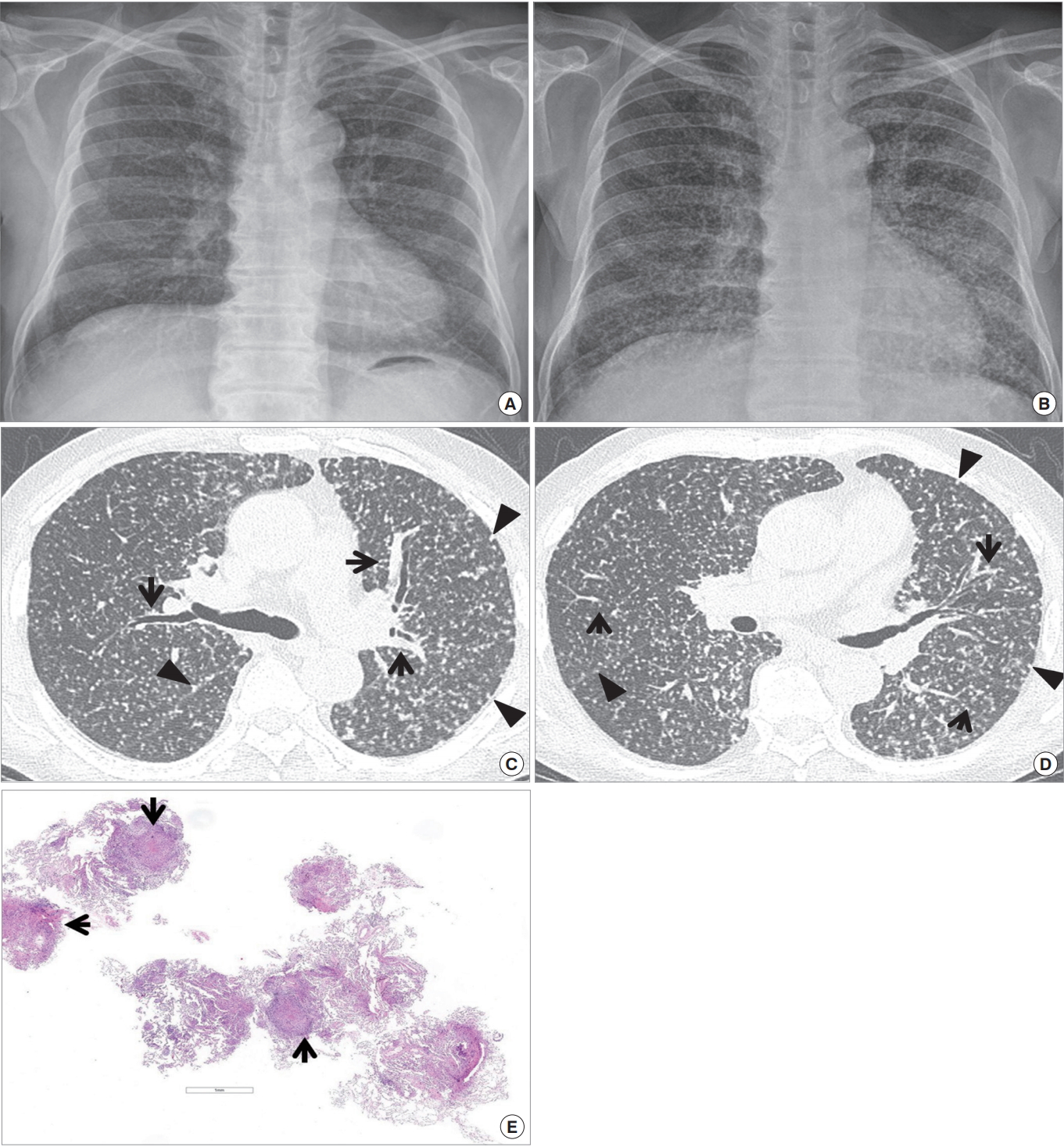
Interstitial pneumonia is characterized histologically by a mononuclear inflammatory cell infiltrate in the alveolar septa and interstitial tissue surrounding small parenchymal vessels (Fig. 5). The most common causes are M. pneumoniae, viruses, and Pneumocystis jirovecii.
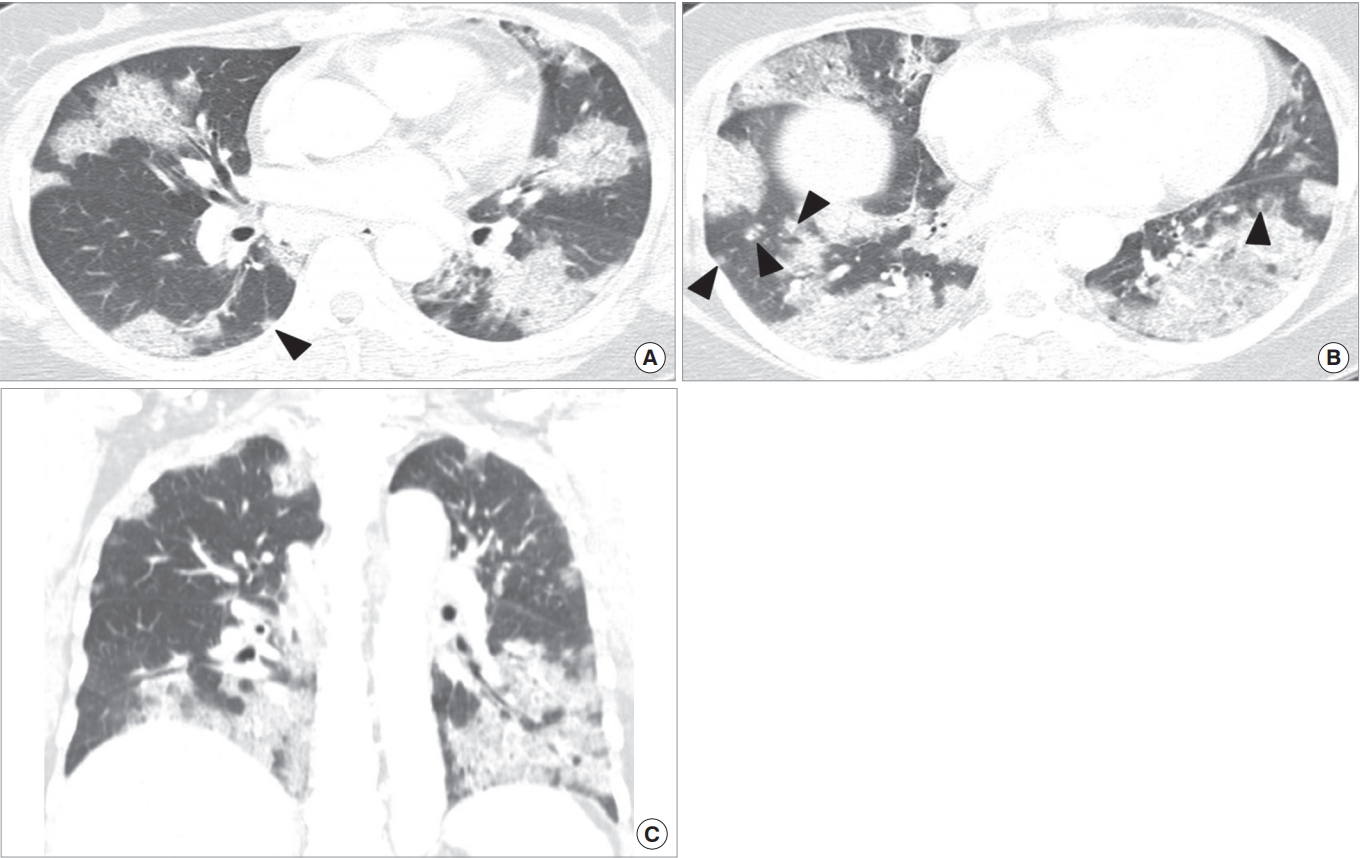
The followings are common pathologic findings in viral pneumonia: viruses can result in several pathologic forms of low respiratory tract infection including tracheobronchitis, cellular bronchiolitis, and pneumonia. Because viral organisms replicate within tissue cells, the most prominent histologic changes are observed in the epithelium and adjacent interstitium. In tracheobronchitis, airway walls are congested and lumen contains mononuclear cell infiltrates. Degeneration and desquamation of the epithelial cells are seen. Cellular (inflammatory) bronchiolitis, particularly important in children, appears with epithelial necrosis, neutrophilic exudate in the airway lumen, and predominantly mononuclear infiltrates in its wall. Parenchymal involvement, the pneumonia, starts with the involvement of the lung adjacent to the terminal and respiratory bronchioles; however, extension throughout the lobule may occur (Fig. 5). Rapidly progressive pneumonia may occur particularly in the elderly and in immunocompromised patients where the lungs histologically show diffuse alveolar damage (Fig. 5) comprising interstitial lymphocyte infiltration, airspace hemorrhage, edema and fibrin, type 2 cell hyperplasia, and hyaline membrane formation [12].
Viral pneumonia manifest radiologically as poorly-defined nodules (airspace nodules of 4 to 10 mm in diameter) and patchy areas of peribronchial GGO and airspace consolidation (Fig. 5). Because of the associated cellular bronchiolitis, hyperinflation is commonly present [12-14]. Progressive pneumonia shows the rapid confluence of consolidation leading to diffuse alveolar damage, consisting of homogeneous or patchy unilateral or bilateral airspace consolidation and GGO or poorly-defined small centrilobular nodules [12].
Pattern approach in pneumonia
The con of pattern approach lies in the fact that such approach helps to design targeted antibiotic treatment or experimental and presumed antibiotic treatment. However, the pros of such approach may include (1) overlap of causative organisms causing a certain pattern of pneumonia, (2) changes in presenting pattern of pneumonia according to patients’ immunity, and (3) changes in the manifesting pneumonia pattern related to pre- or co-existing lung disease.
Pattern approach in diffuse pneumonia
CT parenchymal lung abnormalities in diffuse pneumonia may be classified into three main patterns according to the distribution and patterns of the lung abnormalities; cryptogenic organizing pneumonia (OP) (Fig. 6), acute interstitial pneumonia (AIP) (Fig. 5), and bilateral extensive bronchopneumonia. This classification may help stratify patients with viral pneumonia in terms of their prognoses. In a particular viral pneumonia (influenza A [H1N1] pneumonia), patients with bronchopneumonia pattern have a tendency to belong to the mild illness group, whereas patients with AIP pattern show more severe clinical course in their outcome [8,15,16]. According to one study, CT findings in patients having a mild pneumonia course consist mainly of inflammatory lesions involving large or small airways with focal centrilobular small nodules with tree-in-bud sign and bronchiolar wall thickening [17]. Fatal cases of the same pneumonia present as areas of consolidation with or without GGO on CT scans (AIP pattern) and the abnormalities are pathologically correlated with diffuse alveolar damage [18]. Therefore, it seems that pattern and extent of lung lesions observed at CT in viral pneumonias may be a determining factor for predicting patient’s clinical course and prognosis [8].
The radiologic findings of adult viral pneumonias are variable and overlapping (Table 1). Specific organism diagnosis of a viral pneumonia cannot be made on the basis of imaging features alone. Clinical features such as patient age, immune status, time of year, illness in other family members, community outbreaks, onset, severity, duration of symptoms, and the presence of a rash remain as important aids in diagnosing viral causes of both atypical pneumonia and pneumonia in immunocompromised patients [12].
MIXED PNEUMONIA
Septic pneumonia
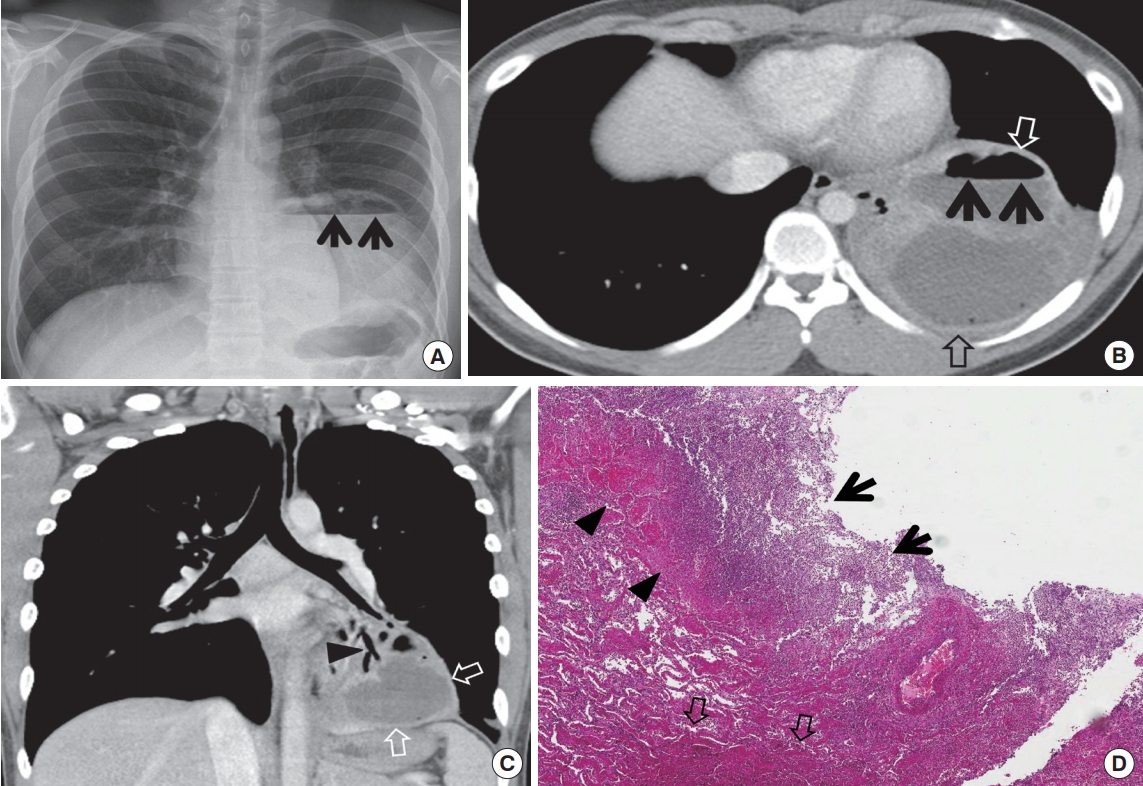
The source of infectious emboli includes infected cardiac valves, septic thrombophlebitis, and infected venous catheter or pacemaker. The pneumonia is caused by the obstruction of pulmonary arteries with infected emboli.
CT findings of septic pneumonia consist of multiple subpleural nodules of 5 to 30 mm in diameter, feeding vessel sign (trace of vessels to the parenchymal lesions [usually nodules]), cavitation of the nodules, air-bronchogram signs within the nodules, and pleural extension of the lesions with effusion (Fig. 7).
K. pneumoniae, S. aureus, and Streptococcus viridans are common organisms isolated in septic pneumonia. Even though the pathogens of septic pneumonia are diverse depending on the primary foci of infection, early diagnosis and prompt antimicrobial therapy can result in successful treatment outcome [19].
Miliary infection
Miliary infection of the lung occurs by seeding of microorganisms present in the blood; free microorganisms per se rather than those in fragments of thrombus as in septic pneumonia. Because the microorganisms are minute in size, they lodge within pulmonary capillaries which are present throughout the whole lung. Spread of the microorganisms to the adjacent alveoli and consequent inflammatory reaction tend to demonstrate the distribution of infection randomly in the lung parenchyma (Fig. 8).
The most common organism responsible for a miliary pattern is Mycobacterium tuberculosis. The small granulomas developing in relation to the minute foci of infection tend to be well delineated, resulting in a distinct nodular appearance both pathologically and radiologically (Fig. 8). The characteristic imaging findings consist of nodule, 1 to 3 mm in diameter, randomly distributed throughout both lungs [20,21].
Lung abscess
Lung abscess is defined as a liquefactive necrotic lung tissue caused by microbial infection where cavities (usually greater than 20 mm in diameter) are contained with necrotic debris and fluid (Fig. 9). The sources of microbial infection include the aspiration of oral flora, necrosis within antecedent pneumonia, central malignancy causing obstructive pneumonia, septic emboli, and penetrating trauma. The common locations of lung abscess are the posterior segment of right upper lobe, superior segment of the right lower lobe, superior segment of the left lower lobe and the posterior basal segment of the left lower lobe (Fig. 9).
Gross pathology shows central suppuration and surrounding wall of fibrous and granulation tissue. On CT, the abscess presents as a cavity with irregular and thick wall (Fig. 9). The cavity wall shows enhancement supplied by the bronchial artery on enhanced scans. The cavity may rupture into the pleural cavity with resultant pleural effusion (usually multiloculated).
In pre-antibiotic era, anaerobes were found in up to 90% of cases, but nowadays they are much less frequent. Aerobic bacteria such as Staphylococcus, Klebsiella, and Hemophilus are also frequently involved. Broad-spectrum antibiotics to cover mixed flora is the mainstay of treatment. Most cases respond to antibiotics and prognosis is usually excellent unless there is a debilitating underlying condition. Mortality from lung abscess alone is around 5% and is improving.
Focal organizing pneumonia
Focal OP is defined as unresolving pneumonia or pneumonia with delayed resolution. With antimicrobial treatment, pneumonia usually resolves within 4 weeks after its initial manifestation on chest radiograph. However, in about 5% to 10% of patients, the pneumonia remains unresolved [22].
Chronic pneumonia
Chronic pneumonia is an illness that lasts at least 6 weeks and is caused by a microorganism. The pneumonias are usually caused by slow-glowing organisms, such as fungi or mycobacteria. Occasionally, chronic pneumonias cannot be diagnosed, even when lung biopsy specimens ware cultured or studied histopathologically [24].
Cryptococcosis
Cryptococcus neoformans is a ubiquitous encapsulated yeastlike fungus that is found worldwide; particularly in soils that are contaminated with pigeon excreta and decayed wood [25]. Inhalation of cryptococcal particles into the lungs is a route of pulmonary infection, and subsequent hematogenous dissemination may cause central nervous system infection [25,26].
Pulmonary cryptococcosis is an indolent lung disease in non-AIDS patients that is slowly progressive in nature, even without adequate treatment. Moreover, it does not show a rapid resolution of the lung abnormalities even with antifungal therapy.
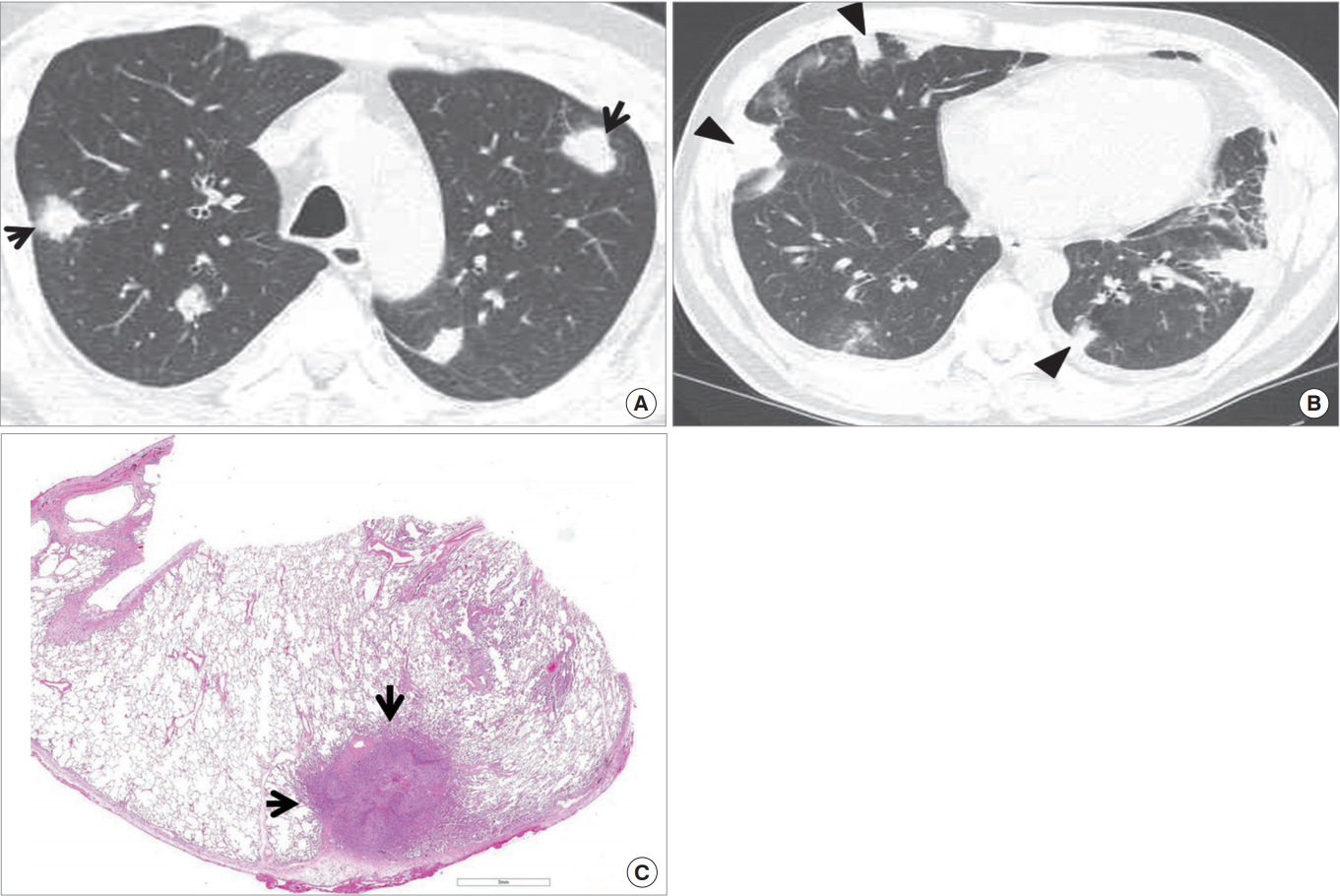
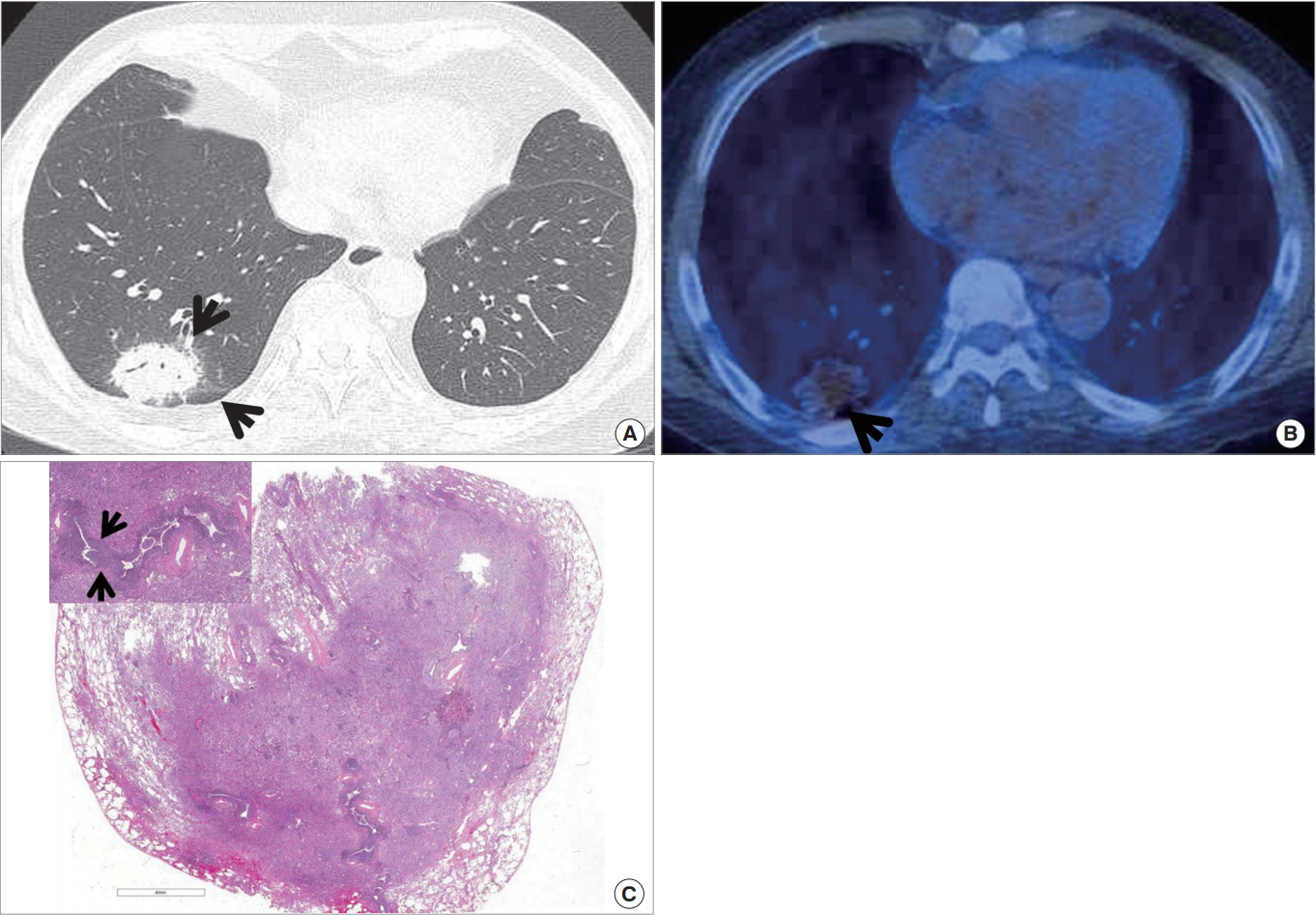
The disease may appear with various patterns of lung lesions; however, a multiple clustered-nodular pattern, localized to a lung lobe, is the most common abnormality (Fig. 11). In half of the cases, the disease appeared in patients with underlying disease, in which most of the patients have an extra-thoracic malignant condition. Therefore, when lung lesions show clustered or scattered nodules of an indolent nature, pulmonary cryptococcosis should be considered in the differential diagnosis, even for a patient with an extrathoracic malignancy. The lesions may show high 18F-fludeoxyglucose (18F-FDG) uptake and may thus simulate a malignant lung condition at positron emission tomography (PET). Although clinical improvement can be achieved in all patients, radiological improvement is slow, even after antifungal therapy. Moreover, lung lesions may persist for a long time, showing a divergence from the clinical response [25].
Actinomycosis
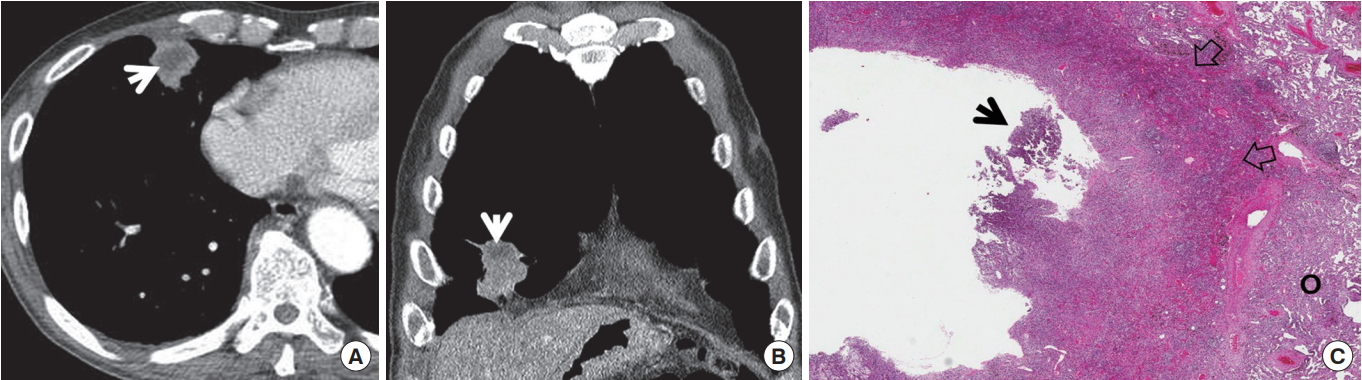
Thoracic actinomycosis is a chronic suppurative pulmonary or endobronchial infection caused by Actinomyces israelii, a gram-positive anaerobic organism. Actinomyces infection typically follows aspiratin of endogenous organisms of the oropharynx into the lungs in persons with poor oral hygiene or from extension of cervicofacial infection. The clinical manifestations of pulmonary actinomycosis are productive cough, low-grade fever, and blood tinged sputum. The prognosis is generally good, provided that the infection is recognized and appropriate antibiotic therapy is instituted [27].
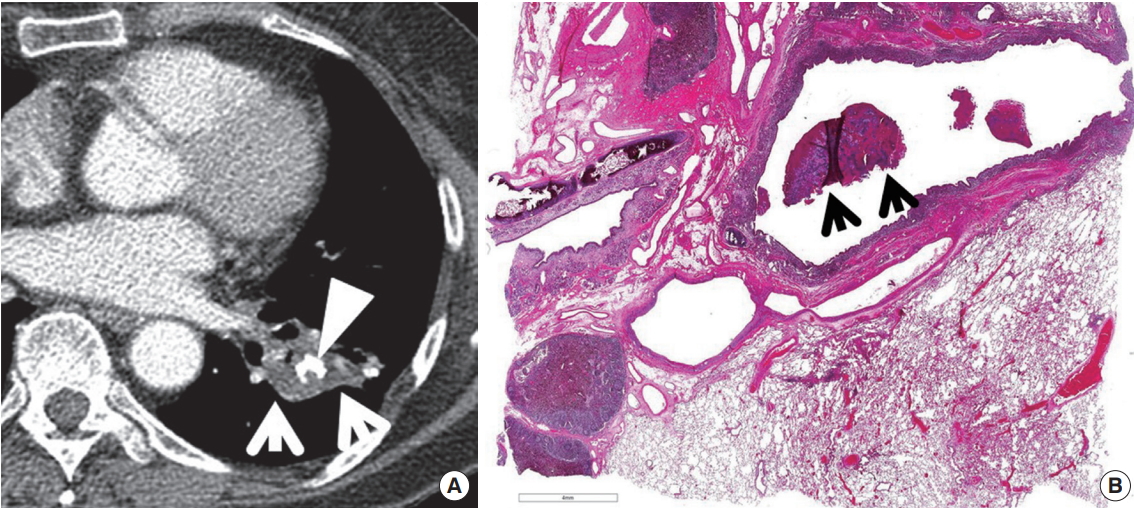
The typical CT feature of parenchymal actinomycosis is a chronic segmental air-space consolidation containing necrotic low-attenuation areas with frequent cavity formation (Fig. 12) [27]. A broncholith can be secondarily infected with Actinomyces organisms, resulting in endobronchial actinomycosis. It usually manifests as a proximal endobronchial calcification associated with distal obstructive pneumonia (Fig. 13) [28].
Chronic pulmonary aspergillosis
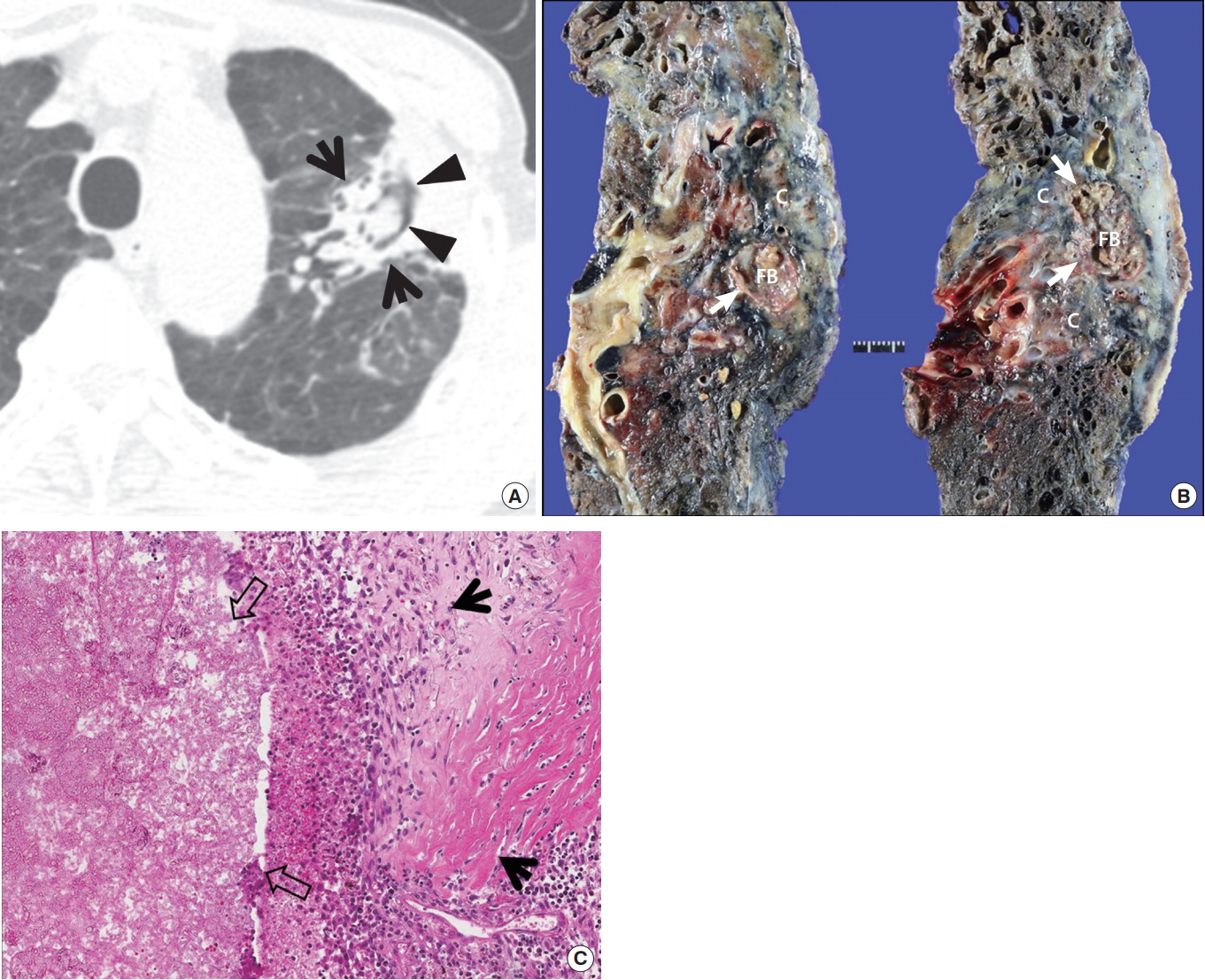
The Infectious Diseases Society of America (IDSA) have proposed three major subtypes of chronic forms of pulmonary aspergillosis, namely chronic necrotizing pulmonary aspergillosis (CNPA; categorized in subacute invasive form of aspergillosis or subacute invasive pulmonary aspergillosis), chronic cavitary pulmonary aspergillosis (CCPA), and aspergilloma [29]. Updated IDSA guidelines have indicated that the differences between CNPA and CCPA include prolonged time frame (CNPA, 1 to 3 months vs. CCPA, > 3 months) (Table 2).
When chronic parenchymal opacity, subsequent progressive cavitation, and consequent aspergilloma formation are serially seen, the diagnosis of CNPA may be made (Fig. 14). Conversely, when pre-existing cavities are subsequently being surrounded by peri-cavitary opacity with or without aspergilloma, the diagnosis of CCPA could be made [30].
Patients with chronic pulmonary aspergillosis are 60 years in their mean age (interquartile range, 45 to 65 years), and show male predominance (approximately 80%). The most common underlying lung disease is pulmonary TB that is seen in more than 90% of the patients [31].
THE ROLE OF IMAGING IN PNEUMONIA
The main role of imaging lies in the detection or exclusion of the presence of pneumonia. Other roles include narrowing down of differential diagnoses of pneumonia regarding causative organisms involved. Further diagnostic approach may be enlightened by observing initial imaging findings. The response to antibiotic therapy may be evaluated by observing follow-up imaging studies.
ANTIBIOTIC THERAPY
Etiologic diagnosis is important for choosing appropriate antibiotics to treat pneumonia. Etiologic diagnosis is often difficult even though the development of imaging and microbiologic diagnostic techniques. Antibiotic treatment should be empirically started against pathogens presumed based on clinical manifestations and imaging patterns before microbiologic results are available. The current paradigm for management of serious hospital-associated infections is to initiate empiric therapy with a broad-spectrum regimen covering likely pathogens, based on local surveillance and susceptibility data, and presence of risk factors for involvement of a resistant microorganism. Subsequent modification (de-escalation) of the initial regimen become possible later, when culture results are available and clinical status can be better assessed, 2 to 4 days after initiation of empiric therapy [32].
Ampicillin, amoxicillin, ceftriaxone, cefotaxime, and respiratory fluoroquinolones (levofloxacin, moxifloxacin) are recommended treatment agents for S. pneumoniae, the most common pathogen causing CAP. Macrolides (azithromycin, clarithromycin) and respiratory fluoroquinolones are treatment options for atypical pneumonia [33]. When fluoroquinolone (a critical component of antituberculous drug regimens for multidrug-resistant TB) is selected, the possibility of TB should be excluded, because exposure to fluoroquinolone prior to the diagnosis of TB has been associated with fluoroquinolone resistance, particularly when the fluoroquinolone exposure occurs > 60 days before TB diagnosis and for longer than 10 days [34].
New antibiotics having activity against pathogens resistant to conventional antibiotics have been developed: anti-MRSA (methicillin-resistant S. aureus) cephalosporins (ceftaroline, ceftobiprole), β-lactams active against resistant Pseudomonas (ceftolozane/tazobactam, ceftazidime/avibactam), new carbapenems (tomopenem, razupenem, imipenem/relebactam), a novel aminomethylcycline agent (omadacycline), etc. Intrapulmonary penetration of antibiotics should be considered in the management of pneumonia. Daptomycin is well known not to be used to treat pneumonia owing to the difficulty of lung penetration of the antibiotics [35]. Regardless of initial antibiotics, coverage should be narrowed down on the basis of susceptibility test results of isolated pathogens.
The conventional 10- to 14-day treatment duration is anecdotal patterns of behavior, not supported by evidence. Recent guidelines recommend 5- to 7-day treatment based on studies showing that a period shorter than 7 days was as effective as longer duration of therapy for mild to moderate CAP [33]. Many adjunctive therapeutic agents including corticosteroids, statins, immunoglobulins, granulocyte colony-stimulating factors, probiotics, and anticoagulants did not show a significant role in pneumonia therapy.
For the viral pneumonia, supportive management is the main therapy. Since several specific antiviral agents are available (oseltamivir or peramivir for influenza, ribavirin for respiratory syncytial virus [RSV], and cidofovir for adenovirus), detection of these viruses is important [36]. Studies on the efficacy of novel antiviral drugs are ongoing.
CONCLUSION
The imaging features of pneumonias caused by various organisms are overlapping. Morphologic classification of pneumonia may help differentiate pneumonias induced by diverse organisms. CT clearly demonstrates the presence of pneumonia and help morphologic classification of the pneumonia. HAP present with complicated imaging findings and should be differentiated from various lung conditions. Chronic indolent nature both in evolution and improvement may suggest the presence of chronic pneumonia such as cryptococcosis, actinomycosis, or CNPA or CCPA. Invasive diagnostic procedure may be needed to make a definite diagnosis of pneumonia and its causative organisms.
New antibiotics having activity against pathogens resistant to conventional antibiotics have been developed. The conventional 10- to 14-day treatment duration is anecdotal patterns of behavior, and recent guidelines recommend 5- to 7-day treatment for mild to moderate CAP with evidencebased studies. Since several specific antiviral agents are available (oseltamivir or peramivir for influenza, ribavirin for RSV, and cidofovir for adenovirus), detection of these viruses is important.