INTRODUCTION
Computed tomography (CT) [1-4] or magnetic resonance imaging (MRI) [5-8] angiography has been accepted for assessing the renal artery and is most commonly performed prior to donor nephrectomy [9-12]. However, this imaging modality is difficult to conduct in patients with poor renal function because intravenous injection of contrast material is essential. Iodine or gadolinium can result in contrast-induced nephrotoxcity toxicity [13-16] or nephrogenic systemic fibrosis [17-20].
Ongoing development of ultrasound (US) scanner technology has improved image resolution so that deep-seated organs can be assessed. Prior to 2000, several investigations reported that US has difficulties in assessing the renal artery for stenosis or obstruction [21-23]. Accordingly, they relied on intra-renal Doppler US in diagnosing renal artery stenosis (RAS) or renal artery obstruction (RAO). Currently, the renal artery can be directly depicted with currently available US scanners [24-27]. RAS or RAO can be precisely identified with renal artery US. This imaging modality does not require CT or MRI contrast material, which should be excreted from the kidney in patients with poor renal function. Even though US contrast materials can be used to assess RAS or RAO, microbubbles can be excreted to the pulmonary circulation [28-31]. Therefore, renal artery US is a safe screening examination for those with suspected RAS or RAO. However, there are few reports about how renal artery US can be applied or its limitations. The purpose of this review is to show clinical applications and diagnostic pitfalls of renal artery US in detecting stenosis or obstruction.
CLINICAL APPLICATIONS
Follow-up of RAS
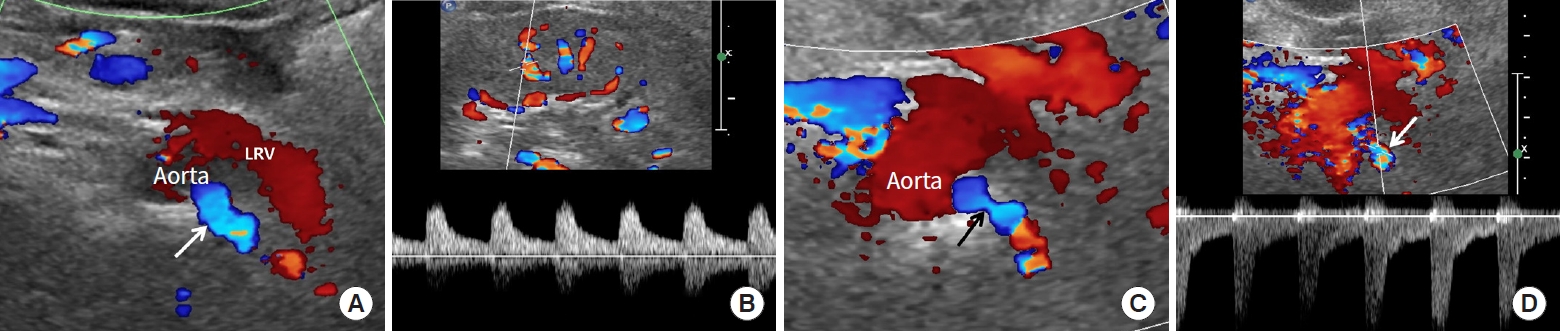
Renal artery US is useful for follow-up after angioplasty [32- 35] or stenting is performed [36-39]. It is important to identify re-stenosis when renal function or blood pressure is not well controlled during the follow-up period. The early stage of re-stenosis does not show pulsus tardus or parvus pattern in the kidney (Fig. 1). Therefore, the renal artery should be carefully evaluated to detect re-stenosis. Color or spectral Doppler US can provide key findings to determine re-stenosis following angioplasty or stenting (Fig. 1). Frequently, a renal artery stent obscures frequency shift from Doppler US due to posterior shadowing. If peak systolic velocity (PSV) is elevated in the renal artery distal to the stent, re-stenosis can be diagnosed. A large decrease in blood flow is another finding suggesting re-stenosis. Contrast-enhanced US can offer added value in depicting blood flow within a stent (Fig. 2).
Poor breath-holding
Breath-holding is necessary to obtain precise Doppler spectrum in the kidney. Accordingly, patient cooperation is essential during renal Doppler US. Many patients with RAS or RAO are old and/or have co-existing morbidities, and it is frequently difficult for them to hold their breath (Fig. 2). However, renal artery US does not require breath-holding for obtaining a renal artery Doppler spectrum (Fig. 2). First of all, the left renal vein should be searched with gray-scale US because renal arteries can be present behind it [24-27]. Then, gray-scale and Doppler US can depict RAS or RAO directly. As RAS becomes severe, the frequency shift is often not sufficient for detection. Thus, post-stenotic dilatation should be determined on a Doppler spectrum (Fig. 1). A PSV greater than 180 to 200 cm/sec in this area [24,40-44] or a PSV reno-aortic ratio (RAR) [44-47] greater than 3.5 strongly suggest RAS. The sensitivity and specificity of PSV > 180 to 200 cm/sec for RAS range from 85%–97% and 72%–98%, respectively [27,42,43,48]. The sensitivity and specificity of RAR > 3.5 for RAS range from 91%– 92% and 71%–95%, respectively [45-47].
Acute kidney injury
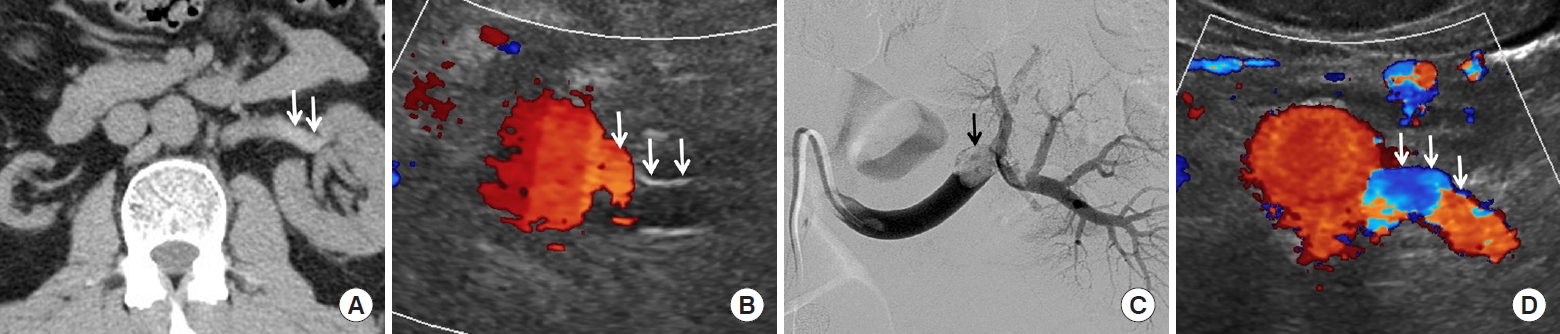
Contrast-enhanced CT or MRI is difficult to perform in patients with acute kidney injury (AKI) because of poor renal function [13-20]. Renal artery US helps to differentiate various conditions resulting AKI (Fig. 3). This US technique can exclude the possibility of RAS as an etiology of AKI. Therefore, if the renal artery is normal, radiologists should evaluate kidney size, echogenicity, perfusion, or obstruction with renal US to determine if AKI is pre-renal, renal, or post-renal [49-51]. For this reason, renal artery or renal US scan is recommended as a primary test for assessing patients with AKI rather than CT or MRI examination. A pre-renal etiology for AKI is most common [51]. The other etiologies include acute tubular necrosis, sepsis, hypovolemia, and drug toxicity [50,52]. Renal artery US helps nephrologists to manage AKI by excluding the likelihood of RAS [49-51].
Guidelines for angio-intervention
Renal artery US can offer good imaging features for detecting early stage RAS, for which angioplasty or stenting is a useful treatment. However, many investigations have reported that this angio-intervention is not as effective in treating chronic stage RAS, and that renal function or renovascular hypertension frequently is aggravated despite angio-intervention [53-56]. Subsequently, radiologists should be familiar with imaging features suggesting early stage RAS. As RAS becomes severe, arterial supply decreases and renal ischemia increases. As a result, cortical echogenicity increases and kidney size decreases. Intra-renal Doppler US shows decreased renal perfusion and pulsus tardus and parvus [57-59]. Early stage RAS can be defined when stenosis is present but kidney size and echogenicity are not significantly changed (Fig. 2). As a result, RAS should be detected before such anatomical changes are clearly depicted on US. When RAS is present in both renal arteries, renal artery US can indicate the treatment priority (Fig. 2). Radiologists should choose a renal artery based on kidney size or echogenicity.
Acute obstruction of renal artery
Acute obstruction of the renal artery results in acute renal infarction and rapid reduction of renal function [60-62]. CT or magnetic resonance angiography is limited for use in patients with poor renal function because of the need for intravenous contrast material. Renal artery US helps to determine RAO resulting from arterial dissection, acute thrombus, or surgical ligation (Fig. 3) [63,64]. These clinical conditions can lead to acute renal failure in patients with single kidney. RAO can occur if the renal artery is ligated during lymph node dissection around the aorta or intravenous vena cava. Early detection with renal artery US can minimize rapid loss of viable renal tissue resulting from acute RAO. Accordingly, this US technique can also help surgeons to determine treatment plans such as re-implantation of renal artery, auto-transplantation, or thrombolysis.
DIAGNOSTIC PITFALLS
Renal artery US has some limitations in assessing stenosis or obstruction. First, in patients with multiple renal arteries, special techniques are needed to detect or assess each renal artery [21-23]. If RAS occurs in the segmental renal artery, beginners might miss it on renal artery US. Even US experts should pay attention to carefully determine the number of renal arteries. If an aberrant renal artery is far from the origin of the main renal artery, it can be difficult to detect.
Second, a PSV greater than 180 to 200 cm/sec or an RAR greater than 3.5 on renal artery US strongly suggest RAS. However, patients with single kidney resulting from nephrectomy have a high PSV or RAR even though RAS is not present [65]. This is a physiologic phenomenon in which a single kidney needs to increase the glomerular filtration rate to match that of two kidneys. Therefore, PSV in a renal artery of a single kidney is almost twice that in paired kidneys immediately after unilateral nephrectomy. This physiologic finding should be differentiated with RAS.
Third, a similar finding can be achieved in the early period of renal allograft. PSV or RAR is higher in the early post-transplantation period than in native renal artery (Fig. 4) [66,67]. Blood flow is markedly elevated in the transplanted renal artery, and pseudo-RAS can be detected in renal artery anastomosis. Because the diameter of the recipient artery is larger than that of the donor artery, anastomosis frequently appears stenotic. Therefore, this anatomical deformity should be differentiated from RAS.
Fourth, renal artery US can detect RAS in the main or segmental renal artery. However, this US technique cannot easily detect small-vessel diseases in the subsegmental renal arteries due to limited image resolution [26]. This limitation is also found in CT or magnetic resonance angiography. Therefore, if small-vessel renal disease is suspected, conventional angiography is a management of choice.
SUMMARY
Renal artery US is useful in assessing poor renal function in patients who have poor breath-holding, follow-up after angio-intervention, screening for AKI, guidelines to angio-intervention, and acute obstruction of the renal artery. However, this US technique has limitations in patients who have multiple renal arteries, single kidney, allograft renal artery, or small-vessel disease.